3154
Views & Citations2154
Likes & Shares
Introduction: Based on the World Health Organization (WHO), viral diseases are emerging and representing one of the crucial issues to the public health. During the past two decades, the organizations have recorded multipleviral epidemics, including H1N1 influenza in 2009 and acute respiratory syndrome coronavirus (SARS-CoV) from 2002 to 2003. In addition, the Middle East respiratory syndrome coronavirus (MERS-CoV) has been initially recognized in Saudi Arabia in 2012. Therefore, in the timetable reaching the present days, the epidemic cases with the unjustified lower respiratory infections discovered in Wuhan, the biggest metropolitan region in Hubei province, China has been firstly announced to the WHO Country Office in China, on December 31, 2019.
Methods: Initially, we searched the research papers using keywords such as WHO, SARS, MERS, COVID-19, pneumonia and treatment of Covid-19. Then, we used WHO data in this article as well as data from the scientific databases such as PubMed, Web of Science and so forth.
Results and Conclusion: Studies in the field have referred to the initiation of the symptomatic people in the early December 2019. Since experts in the field could not determine the causative agent or cause of the disease, they mistakenly categorized the first reported cases as the ‘pneumonia of unknown etiology’. Therefore, the Chinese Center for Disease Control and Prevention (CDC) as well as the local CDCs arranged a concentrated outbreak investigation plan and consequently, this disease etiology has been presently ascribed to one of the newly discovered viruses that are the members of coronavirus (CoV) family or the same COVID-19. In fact, the WHO Director-General, Dr. Tedros Adhanom Ghebreyesus’ reports on February 11, 2020 indicated that the disease caused by this new CoVhas been a ‘COVID-19’; the acronym of ‘coronavirus disease 2019’.
Keywords: COVID-19, MERS, Pneumonia, SARS, WHO
INTRODUCTION
Based on the World Health Organization (WHO), viral diseases are emerging and representing one of the crucial issues to the public health. During the past two decades, the organizations has recorded multiple viral epidemics, including H1N1 influenza in 2009 and acute respiratory syndrome coronavirus (SARS-CoV) from 2002 to 2003. In addition, the Middle East respiratory syndrome coronavirus (MERS-CoV) has been initially recognized in Saudi Arabia in 2012. Therefore, in the timetable reaching the present days, the epidemic cases with the unjustified low respiratory infections discovered in Wuhan, the biggest metropolitan region in Hubei province, China has been firstly announced to the WHO Country Office in China, on December 31, 2019. Therefore, the Chinese Center for Disease Control and Prevention (CDC) as well as the local CDCs arranged a concentrated outbreak investigation plan and consequently, this disease etiology has been presently ascribed to one of the newly discovered viruses, which are the members of the coronavirus (CoV) family or the same COVID-19.
In fact, the WHO Director-General, Dr. Tedros Adhanom Ghebreyesus’ reports on February 11, 2020 indicated that the disease induced by the novel CoV has been a ‘COVID-19 that is an acronym of coronavirus disease 2019'. However, 2 other coronavirus epidemics have been observed during two decades ago. One of the epidemics called SARS-CoV caused one of the large-scale epidemics, which began in China and involved 24 countries with nearly 8000 cases and 800 deaths and the other epidemic called MERS-CoV initiated in Saudi Arabia, accounting for about 2,500 cases and 800 deaths, which still provokes as periodic cases. Apparently, ‘COVID-19’ is largely transmissible and is rapidly spread worldwide. At first, COVID-19 has been termed 2019-nCoV. Then, experts in the International Committee on the Taxonomy of Viruses (ICTV) called it the SARS-CoV-2 virus because of its high similarity to the virus causing SARS outbreak (SARS-CoVs). It has been found that CoVsare the main pathogens of the emerging respiratory disease outbreak. Moreover, these viruses have been considered as one of the large families of the single-stranded RNA viruses (+ssRNA) with the ability of isolation in diverse animal species [1]. However, for reasons that should be clarified, such viruses are able to pass species barriers and create diseases from the common cold to more serious ones like SARS and MERS cause in humans. In addition, possible origination of the former viruses is the bats and subsequently movement into other mammalian hosts-the Himalayan palm civet for SARS-CoV and dromedary camel for MERS-CoV-prior to its jump to the humans. There is not enough information on the SARS-Cov-2 dynamics; however, its animal origin has been speculated. Concerning COVID-19, on February 28, 2020, the WHO reported that there have been ‘very high’ threats caused by the CoV epidemic. Therefore, governments throughout the world are trying to establish some countermeasures for finding the probable destructive impacts. Furthermore, the health organizations share information, directions, and guidelines for further mitigation of the impacts of this threat. Consequently, scientists are constantly working for rapid development of the information of the transmission mechanism, new diagnostic, prevention and therapeutic approaches and clinical spectrum of the disease. However, there would be several uncertainties of the epidemic evolution and virus-host interaction by a particular emphasis on the times when the epidemic reaches its peak. Presently, treatment approaches to address infections have been considered to be merely supportive and prevention with the aim of declining transmission in communities would the most reasonable defense. It is notable that aggressive isolation measures in China caused a progressive diminishment of cases during the past days. On the one hand, in the middle of the crisis, researchers selected the utilization of “Statpearls” platform because it shows a specific device within the PubMed scenario, which could enable them to update in the real time. Thus, the objective has been to collect scientific evidence and information and overview the topic to be continually updated.
DISCUSSION
CoVs are positive-stranded RNA viruses with a crown-like appearance under an electron microscope (coronam is the Latin term for crown) as a result of the presence of the spiked glycoproteins on the envelope. The subfamily Orthocoronavirinae of the Coronaviridae family (order Nidovirales) has been classified into 4 genera of CoVs, including Alphacoronavirus (alphaCoV), Betacoronavirus (betaCoV), Deltacoronavirus (deltaCoV), and finally Gammacoronavirus (gammaCoV). In addition, the betaCoV genus has been divided into five sub-genera or lineages [2]. According to the genomic characterization, the bats and rodents are the probable gene sources of alphaCoVs and betaCoVs. On the contrary, avian species seem to represent the gene sources of deltaCoVs and gammaCoVs. Members of this large family of viruses can cause respiratory, enteric, hepatic and neurological diseases in different animal species, including camels, cattle, cats, and bats. To date, experts in the field identified seven human CoVs (HCoVs) capable of infecting humans. Some of HCoVs were identified in the mid-1960s, while others have been only detected in the new millennium. In general, estimates suggested that 2% of the populations are healthy carriers of a CoV and that these viruses are responsible for about 5% to 10% of acute respiratory infections [3].
· Common human CoVs: HCoV-OC43 and HCoV-HKU1 (betaCoVs of the A lineage), HCoV-229E and HCoV-NL63 (alphaCoVs). These viruses can cause self-limiting upper respiratory infection and common cold in the immuno-competent people. Moreover, lower respiratory tract infections can occur in the immuno-compromised subjects and the elderly.
· Other human CoVs: MERS-CoV (betaCoVs of the B and C lineage, respectively) and SARS-CoV, SARS-CoV-2. These cause epidemics with variable clinical severity, which characterize the respiratory and extra-respiratory manifestations. Concerning SARS-CoV and MERS-CoV, the death rate is up to 10% and 35%, respectively.
Thus, SARS-CoV-2 belongs to the betaCoVs category. It has round or elliptic and often pleomorphic form with a diameter of approximately 60–140 nm. Like other CoVs, it is sensitive to ultraviolet rays and heat. Moreover, these viruses can be effectively inactivated by lipid solvents such as chlorine-containing disinfectant, ethanol, ether (75%), chloroform and peroxyacetic acid except for chlorhexidine. In genetic terms, Chan et al. [4] confirmed that the genome of the new HCoV, isolated from a cluster-patient suffering from the atypical pneumonia following a visit of Wuhan, exhibited 89% nucleotide identity with bat SARS-like-CoVZXC21 and 82% with that of human SARS-CoV. For this reason, the new virus has been called SARS-CoV-2. Its single-stranded RNA genome contains 29891 nucleotides, encoding for 9860 amino acids. Although its origins are not entirely understood, these genomic analyses suggested that SARS-CoV-2 probably evolved from a strain found in bats. However, the potential amplifying mammalian host, intermediate between bats and humans, is not known. Since the mutation in the original strain could directly trigger virulence towards humans, the existence of intermediary is uncertain. Since there has been a relationship between the direct exposures to the Huanan Seafood Wholesale Market of Wuhan and first cases of CoVID-19 disease, animal-to-human transmission has been presumed as the main mechanism. Nevertheless, subsequent cases have been not associated with this exposure mechanism. Therefore, it has been concluded that the virus could also be transmitted from human-to-human, and symptomatic people are the most frequent source of COVID-19 spread. Apparently, possible transmission before the symptom’s development is infrequent, although it cannot be excluded. Moreover, there are suggestions that people without symptoms have been capable of transmitting the virus. This data suggested that the use of isolation would be the best way to contain this epidemic. As with other respiratory pathogens, including flu and rhinovirus, it is believed that transmission occurs through respiratory droplets from coughing and sneezing. Aerosol transmission is also possible in case of the protracted exposure to the elevated aerosol concentrations in closed spaces. Analysis of data related to the spread of SARS-CoV-2 in China indicated that close contact between individuals is one of the important ways affecting the transmission. In fact, the spread is primarily limited to the family members, healthcare professionals and other close contacts. Based on the data from the first cases in Wuhan and investigations conducted by the China CDC and local CDCs, incubation time could be generally within 3 to 7 days and up to 2 weeks as the longest time from infection to symptoms was 12.5 days (95% CI, 9.2 to 18) [5]. This data also showed that this newly detected epidemic doubled about every seven days, whereas the basic reproduction number (R0 - R naught) is 2.2. In other words, on average, each patient transmits the infection to an additional 2.2 individuals. Finally, estimations of the R0 of the SARS-CoV epidemic in 2002-2003 were approximately 3 [6]. It must be emphasized that this information is the result of the first reports. Thus, additional investigations would be needed for understanding the transmission mechanisms, incubation times, clinical course, and duration of infectivity.
EPIDEMIOLOGY
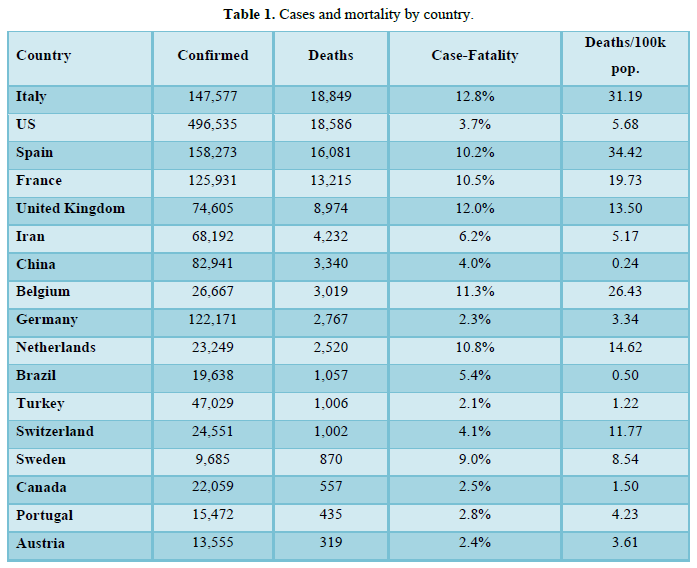
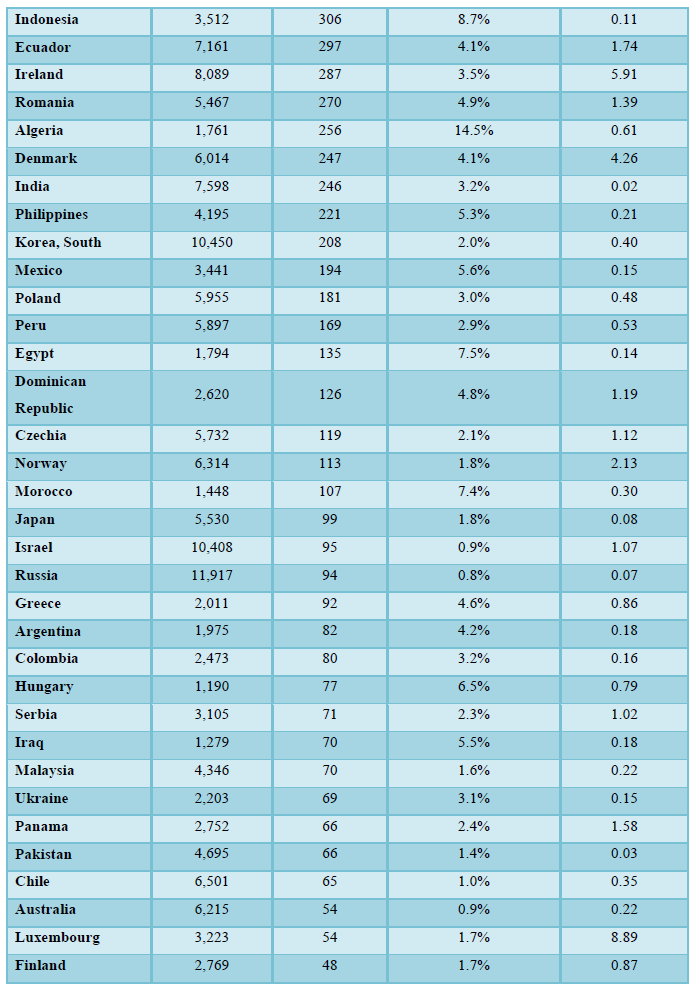
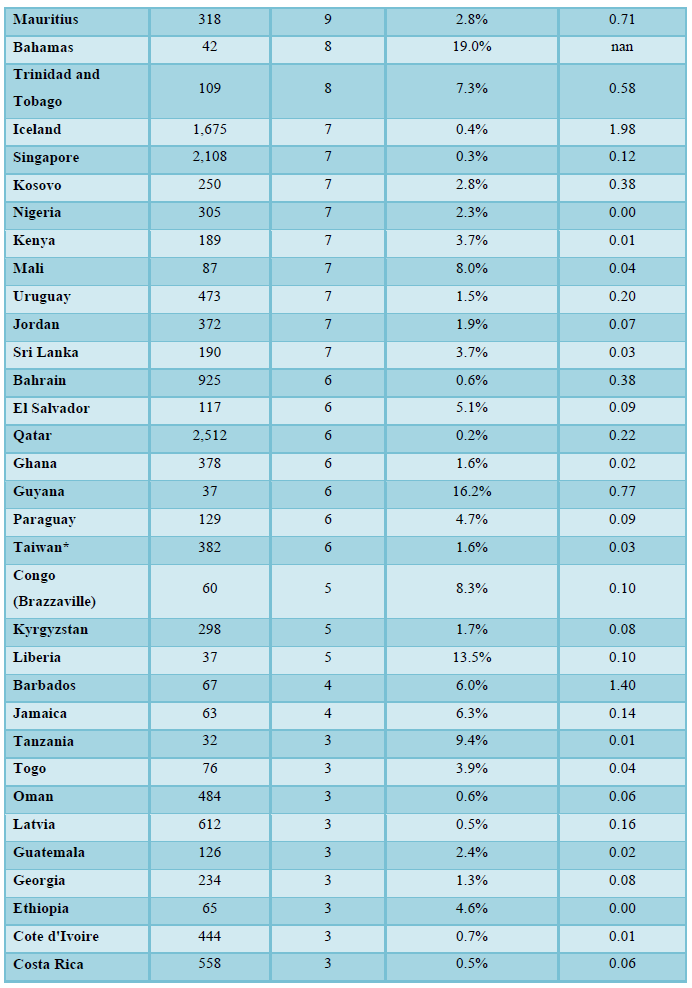
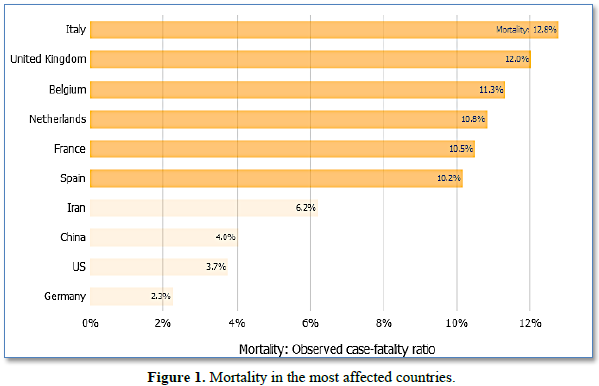
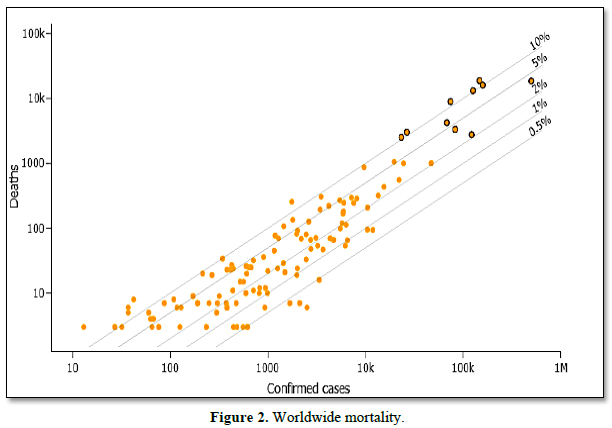
The data obtained from the Johns Hopkins Center for Systems Science and Engineering site for Coronavirus Global Cases COVID-19, which uses openly public sources to track the spread of the epidemic (Data as reported by national authorities by 10:00 CET, 11 April 2020) are presented in Figures 1 and 2, and Table 1.
The most up-to-date source for the epidemiology of this emerging pandemic can be found:
· The WHO Novel Coronavirus (COVID-19) Situation Board, and
· The Center OF Johns Hopkins University for Systems Science and Engineering site for Coronavirus Global Cases COVID-19.
For the 10 countries most affected by COVID-19 worldwide, the bars in the f show the number of deaths either per 100 confirmed cases (observed case-fatality ratio) or per 100,000 population (this represents a country’s general population, with both confirmed cases and healthy people). Countries at the top of this figure have the most deaths proportionally to their COVID-19 cases or population, not necessarily the most deaths overall.
The diagonal lines on the Figure 2 correspond to different case fatality ratios (the number of deaths divided by the number of confirmed cases). Countries falling on the uppermost lines have the highest observed case fatality ratios. Points with a black border correspond to the 10 most affected countries by COVID-19 worldwide, based on the number of deaths. Hover over the circles to see the country name and a ratio value. Use the boxes on the top to toggle between: 1) mortality per absolute number of cases (total confirmed cases within a country); and mortality per 100,000 people (this represents a country’s general population, with both confirmed cases and healthy people).
PATHOPHYSIOLOGY
CoVs are the enveloped, positive-stranded RNA viruses with nucleocapsid. For addressing the pathogenetic mechanisms of SARS-CoV-2, its viral structure and genome should be considered. In CoVs, the genomic structure is organized into a +ssRNA of approximately 30 kb in length, which is the biggest identified RNA viruses, with a 3′-poly-A tail and 5′-cap structure. Starting from viral RNA, the synthesis of polyprotein 1a/1ab (pp1a/pp1ab) in the host is realized. Transcription works through the replication-transcription complex (RCT) organized into the double-membrane vesicles and synthesis of the subgenomic RNAs (sgRNAs) sequences. It should be noted that transcription terminates at the transcription regulatory sequences, located between the so-called open reading frames (ORFs) that work as the templates to produce the sub-genomic mRNAs. In atypical CoV genome, at least six ORFs can be present. Among these, a frame-shift between ORF1a and ORF1b guides the generation of both pp1a and pp1ab poly-peptides that have been processed by the virally encoded chymotrypsin-like protease (3CLpro) or the main protease (Mpro), as well as 1 or 2 papain-like proteases for producing 16 non-structural proteins (nsps). Apart from ORF1a and ORF1b, other ORFs encode for the structural proteins, including membrane, spike, nucleocapsid proteins, envelope [1] and accessory proteic chains. Various CoVs present the special accessory and structural proteins translated by the dedicated sgRNAs. According to the analyses, pathophysiology, virulence mechanisms of CoVs and SARS-CoV-2 are linked to the function of nsps and structural proteins. For instance, research emphasized that nspcan block the host innate immune response [7]. Among functions of structural proteins, the envelope has a crucial role in the virus pathogenicity as it promotes viral assembly and release. However, many of these features (e.g., those of nsp 2 and 11) have not yet been described. Among the structural elements of CoVs, there is the spike glycoproteins composed of two subunits (S1 and S2). Homo-trimers of S proteins contain the spikes on the viral surfaces, guiding the link to the host receptors [8]. Moreover, in SARS-CoV-2, the S2 subunit, which contains a fusion peptide, a transmembrane domain, and cytoplasmic domain, is highly conserved. Thus, it could be a target for antiviral (anti-S2) compounds. On the contrary, the spike receptor-binding domain presents only a 40% amino acid identity with other SARS-CoVs. Other structural elements on which the research should necessarily focus are the ORF3b that has no homology with that of SARS-CoVs and a secreted protein (encoded by ORF8), which is structurally different from those of SARS-CoV. In the international gene banks such as GenBank, researchers have published several Sars-CoV-2 gene sequences. This gene mapping is of fundamental importance so that it allows researchers to trace the phylogenetic tree of the virus and, above all, the recognition of strains that differ according to the mutations. Based on a recent research, a spike mutation, which probably occurred in the late November 2019, triggered jumping to humans. In particular, Angeletti et al. [9] compared the Sars-Cov-2 gene sequence with that of SARS-CoV. They analyzed the transmembrane helical segments in the ORF1ab encoded 2 (nsp2) and nsp3 and found that position 723 presents a serine instead of a glycine residue, while the position 1010 is occupied by proline instead of isoleucine. Therefore, the issue of viral mutations is key for explaining the potential disease relapses. Hence, some studies will be needed to determine the structural characteristics of SARS-COV-2 that focus on the pathogenetic mechanisms. Compared to SARS, initial clinical data showed less extra respiratory involvement, although it is not possible to draw definitive clinical information due to the lack of extensive data.
HISTOPATHOLOGY
Tian et al. [10] reported histopathological data obtained on the lungs of two patients who underwent lung lobectomies for adenocarcinoma and retrospectively found their infection at the time of surgery. Apart from the tumors of the lungs of both ‘accidental’ cases showed edema and important proteinaceous exudates as large protein globules. The authors also reported vascular congestion combined with inflammatory clusters of fibrinoid material, multinucleated giant cells, and hyperplasia of pneumocytes.
HISTORY AND PHYSICAL CHARACTERISTICS
The clinical spectrum of COVID-19 varies from asymptomatic or paucisymptomatic forms to the clinical conditions characterized by respiratory failures, which necessitates mechanical ventilation as well as supports in an intensive care unit (ICU), to multiorgan and systemic manifestations in terms of sepsis, multiple organ dysfunction syndromes (MODS), and septic shock. According to one of the first reports on the disease, Huang et al. [11] illustrated that patients (n=41) suffered from fever, malaise, dry cough and dyspnea. In addition, the chest computerized tomography (CT) scans showed pneumonia with abnormal findings in all cases. About a third of those (13: 32%) required ICU care and 6 (15%) fatal cases have been reported. Moreover, Li et al.’s [5] case study reported in the New England Journal of Medicine (NEJM) on January 29, 2020 encapsulated the first 425 cases recorded in Wuhan. According to the data, the patients’ median age has been 59 years in the range of 15 to 89 years. These researchers reported no clinical cases in children >15 years of age. Furthermore, no significant gender differences (56% male) have been observed. Clinical and epidemiological data from the Chinese CDC and with regard to 72,314 case records (confirmed, suspected, diagnosed, and asymptomatic cases) have been shared in the Journal of the American Medical Association (JAMA) (February 24, 2020) and provided an important illustration of the epidemiologic curve of the Chinese outbreak [12]. There have been 62% confirmed cases, including 1% of cases that have been asymptomatic, but laboratory-positive (viral nucleic acid test). Consequently, the overall case-fatality rate (on the confirmed cases) equaled 2.3%. As a result, the fatal cases have been primarily observed in the elderly patients, in particular, those aged ≥80 years (about 15%) and 70 to 79 years (8.0%). Approximately half (49.0%) of the critical patients and affected by the pre-existing comorbidity like cardio-vascular disease, chronic respiratory disease, oncological diseases, and diabetes died due to the disease. While 1% of the patients aged 9 years or younger and no fatal cases occurred in this group.
It is notable that the authors of the Chinese CDC report divided the clinical manifestations of the disease by their severity:
· Mild disease: Non-pneumonia and mild pneumonia that occurred in 81% of cases.
· Severe disease: Dyspnea, respiratory frequency ≥ 30/min, and blood oxygen saturation. (SpO2) ≤ 93%, PaO2/FiO2 ratio [the ratio between the blood pressure of the oxygen (partial pressure of oxygen, PaO2) and the percentage of the oxygen supplied (fraction of the inspired oxygen, FiO2)] < 300, and/or lung infiltrates > 50% during 24-48 h that occurred in 14% of cases.
· Critical disease: Septic shock, multiple organ dysfunction (MOD) or failure (MOF) and respiratory failure that occurred in 5% of cases [12].
Data obtained from the reports and directives provided by the health policy agencies allowed the division of the clinical manifestations of the disease according to the severity of the clinical pictures. It has been found that COVID-19 may exhibit with the mild, moderate, or severe disease. Among these serious clinical manifestations, there are acute pneumonia, sepsis, septic shock and ARDS. On the one hand, clinical course of the disease seems to predict a favorable trend in the majority of patients so that a sudden worsening of the clinical conditions with the rapidly worsening respiratory failure and MOD/MOF has been observed after about a week. Finally, the criteria of the severity of the respiratory insufficiency and diagnostic criteria of sepsis and septic shock can be used as a reference [13].
Uncomplicated (mild) illness
These patients usually exhibit symptoms and signs of an upper respiratory tract viral infection, including mild fever, cough (dry), nasal congestion, headache, malaise, sore throat and muscles pain, or malaise. However, symptoms of a more serious disease, such as dyspnea, have been not observed. Compared to the previous HCoV infections, it is a challenge to find the non-respiratory symptoms such as diarrhea.
Moderate pneumonia
Moreover, respiratory symptoms such as cough and shortness of breath (or tachypnea in children) are reported without signs of severe pneumonia.
Severe pneumonia
Fever is associated with severe dyspnea, respiratory distress, tachypnea (>30 breaths/min), and hypoxia (SpO2<90% on room air). However, the fever symptom must be interpreted carefully because it can be moderate or even absent even in the serious or acute forms of illness. Cyanosis can occur in children. In this definition, the diagnosis is clinical, and radiologic imaging is used for excluding complications.
Acute Respiratory Distress Syndrome (ARDS)
It is widely accepted that diagnosis requires clinical and ventilatory criteria. This syndrome suggests a serious new-onset respiratory failure or for worsening of an already identified respiratory picture. Therefore, different forms of ARDS are distinguished based on the degree of hypoxia. The reference parameter is the PaO2/FiO2:
· Mild ARDS: 200 mmHg
· Moderate ARDS: 100 mmHg
· Severe ARDS: PaO2/FiO2≤100 mmHg.
Notably, in case of unavailability of PaO2, a ratio of SpO2/FiO2 ≤ 315 would suggest ARDS.
In addition, chest imaging includes chest radiograph, lung ultrasound and CT scan, demonstrating the bi-lateral opacities (lung infiltrates >50%), which would not be thoroughly illustrated by lobar, lung collapse, or effusion. Although in some cases, the clinical scenario and ventilator data could indicate pulmonary edema, the primary respiratory origin of the edema is proven after excluding cardiac failure or other causes such as fluid overload. Hence, echocardiography can be helpful for this purpose.
Sepsis
In accordance with the International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3), sepsis represents a very dangerous organ dysfunction induced by the dysregulated host responses to the suspicious or proven infections, with organ dysfunction [14]. On the other hand, clinical pictures of patients affected by COVID-19 and sepsis are particularly serious, characterized by a wide range of signs and symptoms of multiorgan involvement. These symptoms include respiratory manifestations such as severe dyspnea and hypoxemia, renal impairment with the reduced urine output, tachycardia, altered mental status and functional alterations of organs expressed as the laboratory data of hyperbilirubinemia, acidosis, high lactate, coagulopathy, and thrombocytopenia. It is notable that the Sequential Organ Failure Assessment (SOFA) score is the reference for the evaluation of multiorgan damage and the related prognostic significance, which anticipates ICU mortalities on the basis of the lab outputs and clinical information [15]. Finally, validity of a pediatric version of the score has been confirmed [16].
Septic shock
In this scenario, which is associated with the increased mortality, circulatory and cellular/metabolic abnormalities such as the levels of serum lactate higher than 2 mmol/L (18 mg/dL) have been reported. Since patients usually suffer from the persisting hypotension despite volume resuscitation, it is necessary to administer vasopressors for maintaining a mean arterial pressure (MAP) higher than or equal to 65 mmHg.
TREATMENT AND MANAGEMENT
According to the studies, no specific antiviral treatment for COVID-19 has been recommended and, no vaccine is currently available. Treatment is symptomatic and oxygen therapy represents a main therapeutic intervention for patients suffering from severe infection. In addition, mechanical ventilation may be necessary in cases of respiratory failure refractory to oxygen therapy, whereas hemodynamic support is essential for managing the septic shock. With regard to the early in vitro studies, chloroquine blocked COVID-19 infection at low micro-molar concentration, with a half-maximal effective concentration (EC50) of 1.13 μM and a half-cytotoxic concentration (CC50) higher than 100 μM [17]. Therefore, authors quickly conducted some subsequent clinical trials in China for testing the effectiveness and safeness of chloroquine or hydroxychloroquine for treating the COVID-19 related pneumonia in higher than ten hospitals in Jingzhou, Wuhan, Beijing, Guangzhou, Chongqing, Ningbo and Shanghai [18]. Furthermore, outputs obtained from above 100 patients revealed the superiority of chloroquine phosphate over the control treatment for inhibition of exacerbated pneumonia, which ameliorated the lung imaging results, promoted a virus-negative conversion and shortened the disease course based on the news briefing. Consequently, authors observed serious bad reactions to chloroquine phosphate in the above patients. With regard to the outcomes, a conference has been held on February 15, 2020 and people participating in the conference like the experts from stateas well as regulatory authorities and organizers of the clinical trials made consensus of the potential activities of chloroquine phosphate against COVID-19. This medicine has been advised to be included in the next version of Guidelines for Prevention, Diagnosis, and Treatment of Pneumonia Induced by COVID-19 released by the National Health Commission of the People’s Republic of China. Chloroquine has been considered to be utilized for the prevention and treatment of malaria and has been confirmed as an effective drug as one of the anti-inflammatory agents to treat lupus erythematosus and rheumatoid arthritis. However, investigations illustrated its potential wide spectrum antiviral activity via enhancing the endosomal pH needed for virus and cell fusion and intervening with glycosylation of the cellular receptors of SARS-CoV [19,20] The antiviral and anti-inflammatory activity of chloroquine can demonstrate its potential efficiency to treat the patients suffering from COVID-19 pneumonia. In addition, chloroquine has been considered one of the inexpensive and safe drugs utilized for above 70 years [21]. Regarding crucial clinical demands, chloroquine phosphate has been advised for treating the COVID-19-related pneumonia in larger populations in the future. In order to diagnose COVID-19, though RT-qPCR is specific, its false-negative rate could not be neglected due to very bad effects of the missed diagnosis. Therefore, multiple clinicians introduced CT scan as a crucial auxiliary diagnostic approach due to its higher sensitivity. In addition, the combined frequent RT-qPCR tests and chest CT scans could be beneficial for people with highly clinical suspected SARS-CoV-2 infections with negative RT-qPCR screening. In particular, high-resolution CT (HRCT) for the chests would be required to initially diagnose and evaluate the disease acuteness in the patients affected by SARS-CoV-2. In this regard, numerous investigations examined the CT images of the patients' chests infected with SARS-CoV-2. Characteristic CT images showed consolidative pulmonary opacities as well as bi-lateral pulmonary parenchymal ground-glass, occasionally with a peripheral lung distribution and rounded morphology. It is notable that the lungs’ involvement with a peripheral predominance has been observed in patients with MERS-CoV and SARS-CoV infections. Moreover, chests CTs indicated the disease progression with the ground-glass opacity and consolidation that is the same as the SARS-CoV-2 infection. It has been found that the CT scans showed a very clinical diagnostic significance for COVID-19, specifically in a high prevalence area of SARS-CoV-2 infections. Nonetheless, CT scans suffer from a number of caveats like in-distinguishability from other viral pneumonia and hysteresis of abnormal CT imaging. With regard to the disadvantage of the newly applied nucleic acid detection and CTs to diagnose COVID-19, it is necessary for the clinical laboratories to utilize a number of immunological detection kits, which immediately targeted the viral antibodies or antigens. As a result, a number of companies in the field devised and pretested POCT of IgM/IgG and ELISA kits for SARS-CoV-2 and showed greater rate of detection in comparison to the nucleic acid detection, though any products or articles have been not yet reported. On the other hand, sensitivity of SARS-CoV N-based IgG ELISA (94.7%) has been considerably greater than that of the SARS-CoV S-based IgG ELISA (58.9%); however, SARS-CoV-2 IgG/IgM sensitivity should be investigated. Ultimately, it is necessary to develop additional specific and sensitive auxiliary techniques to diagnose COVID-19.
DIFFERENTIAL DIAGNOSIS
According to the analyses, symptoms of the early stages of the disease are non-specific and thus differential diagnosis should include the possibility of a wide range of infectious and non-infectious (e.g., vasculitis and dermatomyositis) common respiratory disorders.
• Adenovirus,
• Influenza,
• Human metapneumovirus (HmPV),
• Parainfluenza,
• Respiratory syncytial virus (RSV), and
• Rhinovirus (common cold)
Moreover, for the suspected cases, rapid antigen detection and other investigations should be adopted for evaluating common respiratory pathogens and non-infectious conditions.
DETERRENCE AND PATIENT EDUCATION
Patients and families should receive the following instructions:
Ø Persons should avoid the close contacts with the individuals having acute or severe respiratory infection.
Ø People should wash their hands regularly, in particular, following the contacts with sick persons or the respective environments.
Ø People should stop the unprotected contacts with farms or wild animals.
Ø Persons having the symptoms of serious airway infections should keep their distances, cover coughing or sneezing with disposable clothes and tissues, and wash frequently their hands.
Ø Moreover, immunocompromised patients should avoid public exposure and public gatherings. If an immunocompromised individual must be in a closed space with multiple individuals present, such as a meeting in a small room; masks, gloves, and personal hygiene with antiseptic soap should be undertaken by those in close contact with the individual. In addition, prior room cleaning with antiseptic agents should be prioritized and performed before exposure. However, with regard to the dangers involved to these individuals, exposure should be avoided unless a meeting, group event, and the like is a true emergency.
Ø Strict personal hygiene measures are necessary for prevention and control of this infection.
CONCLUSION
According to the analyses, incidence and development of SARS-CoV-2 are depended on the interactions between virus and humans’ immune systems. In fact, viral parameters included the kind of virus, viral load and titer, viability of the virus in vitro and mutation. Moreover, immune system parameters of humans included age, genetics (e.g., HLA genes), gender, neuro-endocrine-immune regulation, physical status and nutrition. Therefore, all of the mentioned parameters play a role in of one person would be infected with the virus and duration and severity of the disease, as well as reinfection or not. However, during the initial phases of the epidemic, precise diagnosis contributes to the control of the disease spread or expansion. Hence, development of a novel, safe, precise, rapid and easy technology should be prioritized to detect SARS-CoV-2. In addition, doctors would, physicians would deliberately apply interventions in both parameters for developing them into a path helpful to human health so that they would assist the fast recovery of the patients. Nonetheless, it should be kept in mind that medical interventions could obtain a 100% curative effect.
ACKNOWLEDGEMENT
Hereby, we acknowledge and thank God for giving us the gift of mind. We also kindly express our gratitude to the martyr Qasem Soleimani.
FINANCIAL SUPPORTS AND SPONSORSHIPS
Researchers of the present research financially supported their study.
AUTHORS’ CONTRIBUTION
We declare that the present research has been conducted by the researchers mentioned in the paper and each liability related with the claims on the paper contents has been up the researchers.
ETHICAL APPROVAL
Researchers of the present research did not involve any investigations with the human participants or animals.
1. Perlman S, Netland J (2009) Coronaviruses post-SARS: Update on replication and pathogenesis. Nat Rev Microbiol 7:439-50.
2. Chan JF, To KK, Tse H, Jin DY, Yuen KY (2013) Interspecies transmission and emergence of novel viruses: Lessons from bats and birds. Trends Microbiol 21: 544-555.
3. Chen Y, Liu Q, Guo D (2020) Emerging coronaviruses: Genome structure, replication, and pathogenesis. J Med Virol 92: 418-423.
4. Chan JF, Kok KH, Zhu Z, Chu H, To KK, et al. (2020) Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect 9: 221-236.
5. Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med.
6. Bauch CT, Lloyd-Smith JO, Coffee MP, Galvani AP (2005) Dynamically modeling SARS and other newly emerging respiratory illnesses: Past, present, and future. Epidemiology 16: 791-801.
7. Lei J, Kusov Y, Hilgenfeld R (2018) Nsp3 of coronaviruses: Structures and functions of a large multi-domain protein. Antiviral Res 149: 58-74.
8. Song W, Gui M, Wang X, Xiang Y (2018) Cryo-EM structure of the SARS coronavirus spike glycoprotein in complex with its host cell receptor ACE2. PLoS Pathog 14: e1007236.
9. Angeletti S, Benvenuto D, Bianchi M, Giovanetti M, Pascarella S, et al. (2020) COVID-2019: The role of the nsp2 and nsp3 in its pathogenesis. J Med Virol.
10. Tian S, Hu W, Niu L, Liu H, Xu H, et al. (2020) Pulmonary pathology of early phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. J Thorac Oncol.
11. Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395: 497-506.
12. Wu Z, McGoogan JM (2020) Characteristics of and Important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA.
13. Kogan A, Segel MJ, Ram E, Raanani E, Peled-Potashnik Y, et al. (2019) Acute Respiratory Distress Syndrome following cardiac surgery: Comparison of the American-European consensus conference definition versus the Berlin Definition. Respiration 97: 518-524.
14. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, et al. (2016) The third International Consensus Definitions for sepsis and septic shock (Sepsis-3). JAMA 315: 801-810.
15. Seymour CW, Kennedy JN, Wang S, Chang CH, Elliott CF, et al. (2019) Derivation, validation and potential treatment implications of novel clinical phenotypes for sepsis. JAMA 321: 2003-2017.
16. Matics TJ, Sanchez-Pinto LN (2017) Adaptation and validation of a pediatric sequential organ failure assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatr 171: e172352.
17. Wang M, Cao R, Zhang L, Yang X, Liu J, et al. (2020) Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res 30: 269-271.
18. CHICTR (2020) Chinese Clinical Trial Registry.
19. Savarino A, Boelaert JR, Cassone A, Majori G, Cauda R, et al. (2003) Effects of chloroquine on viral infections: An old drug against today's diseases? Lancet Infect Dis 3: 722- 727.
20. Yan Y, Zou Z, Sun Y, Li X, Xu KF, et al. (2013) Anti-malaria drug chloroquine is highly effective in treating avian influenza A H5N1 virus infection in an animal model. Cell Res 23: 300-302.
21. Zlojutro A, Rey D, Gardner L (2019) Optimizing border control policies for global outbreak mitigation. Sci Rep 9: 2216.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Spine Diseases
- Oncology Clinics and Research (ISSN: 2643-055X)
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Dermatology Clinics and Research (ISSN:2380-5609)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)



