
59
Views & Citations10
Likes & Shares
Recent reports suggest that hormone replacement therapy may be effective not only for arthropathy of the hands in middle-aged women (2), but also for larger joints, including the elbows, shoulders, hips (3), knees (4), and ankles. In the present case, although the patient initially experienced generalized joint pain, initiation of HRT led to sufficient symptomatic improvement to allow her to resume work without difficulty.
METHOD
Definition of menopause
Clinically, the patient had experienced amenorrhea for one year. Serum hormone testing showed an estradiol (E2) level at the lower limit of 20 pg/mL and a follicle-stimulating hormone (FSH) level exceeding 40 mIU/mL.
SMI (Simplified Menopausal Index)
The severity of menopausal symptoms was evaluated using the Simplified Menopausal Index (SMI) (5). An SMI score of 51 or higher indicates the presence of significant menopausal symptoms and identifies patients who may benefit from therapeutic intervention.
Conventional HRT (hormone replacement therapy
A standard cyclical intermittent regimen was employed. The monthly schedule consisted of 0.72 mg estrogen patches applied for 14 days, followed by 12 days of estrogen patches combined with 10 mg of oral dydrogesterone, and then a 5-day drug-free interval.
CONSENT
Written informed consent was obtained from the patient for the publication of this case report.
RESULTS
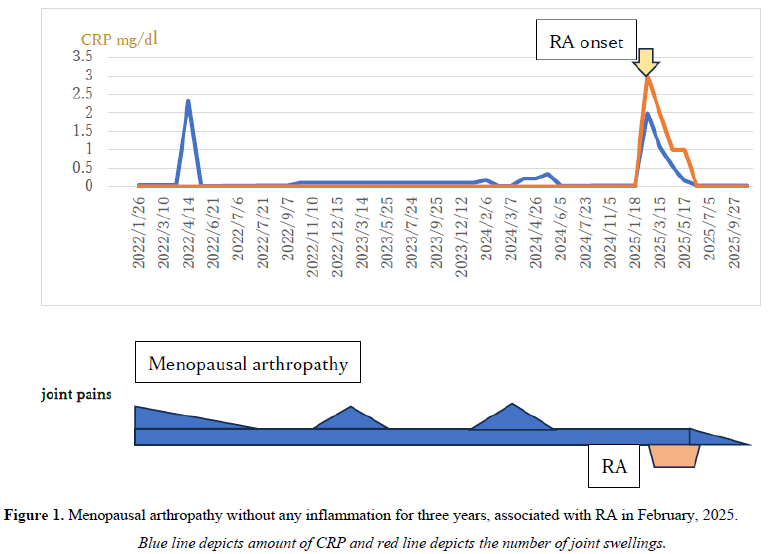
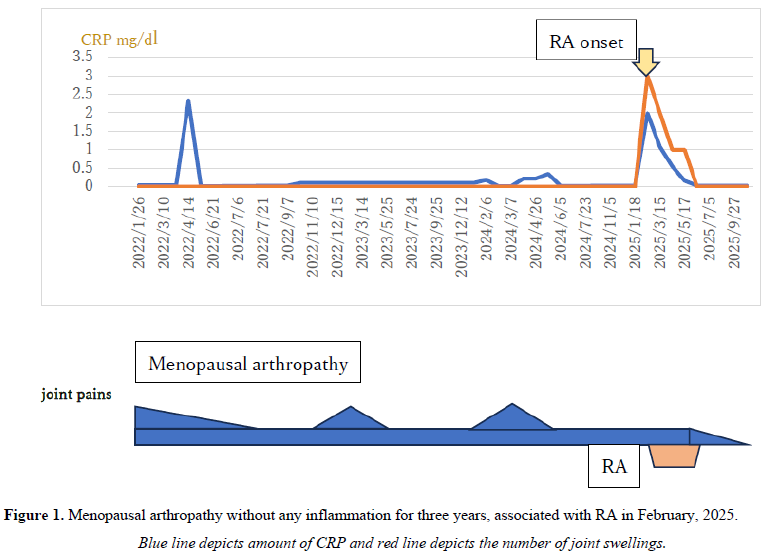
Abrupt RA occurrence proved by elevation of CRP and synovial swelling and tenderness
In April 2022, the patient experienced a transient elevation of CRP (2.3 mg/dL), which normalized by the following month. From February to April 2024, mild CRP elevations were noted, although the underlying cause remained unclear. Despite persistent motion-related joint pain throughout her body, laboratory tests revealed no elevation of CRP or MMP3. In February 2025, two months after her initial visit to our hospital, the patient developed rapid onset redness and swelling in multiple MCP joints, confirming the diagnosis of RA (Figure 1).
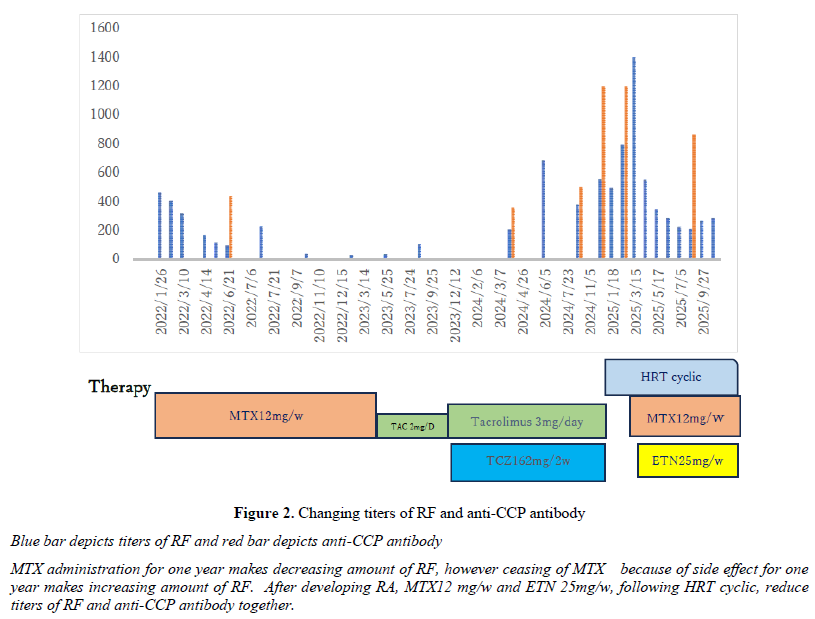
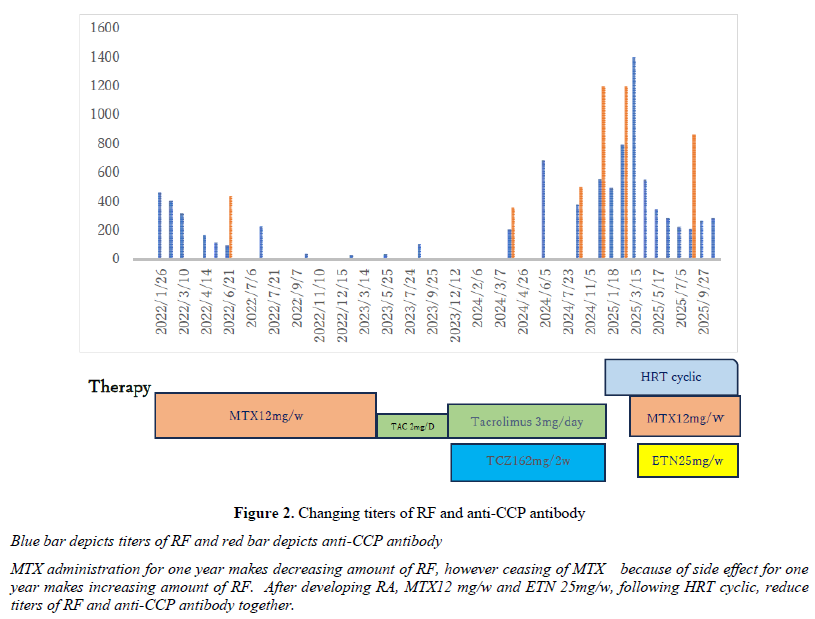
Changing of serological markers of RA during the MTX and biologic agents’ treatment
Since January 2022, the patient had been receiving MTX 12 mg/w, resulting in a marked decrease in RF from 463 units to 33 units over approximately one year. However, due to MTX-related adverse effects, the patient was transitioned to alternative immunosuppressants and biologic therapies, during which RF and anti-CCP antibody levels increased. At her first visit to our clinic on December 21, 2024, laboratory evaluation revealed RF 556 units and anti-CCP antibodies 1200 units, with serum E2 below 20 pg/mL and FSH at 80 mIU/mL. Cyclical HRT was initiated for the prevention of RA.
In March 2025, CRP rose to 1.99 mg/dL, and the patient developed swelling and redness in MCP joints, consistent with the onset of RA. MTX 12 mg weekly was promptly reinstated, followed by ETN 25 mg weekly the subsequent month. By June 2025, RF had decreased to 226 units, and CRP normalized to 0.03 mg/dL. As of October 2025, CRP remains low, and both tendonitis and active synovitis associated with RA have completely resolved (Figure 2).
DISCUSSION
In this case, the patient received a score of 3 for both RF and anti-CCP antibodies due to strong positivity, 0 for CRP negativity, 1 for persistent joint pain lasting more than six weeks, and 5 for pain and tenderness in 11 or more affected joints, yielding a total score of 9 according to the EULAR/ACR classification criteria for RA (6). However, the assessment of affected joints at previous hospitals appears to have been inconsistent. The patient reported no joint swelling, and CRP levels never exceeded 0.3 mg/dL, suggesting absence of synovial thickening. Tendon thickening was observed at the base of the fingers on the palmar side, and carpal tunnel syndrome with associated tenderness could have been misinterpreted as wrist synovitis. While differentiating osteoarthritis or Bouchard’s nodes from bone erosion due to RA on joint ultrasound can be challenging, distinguishing tendonitis from synovitis is relatively straightforward. Based on these findings, this case is considered a 4-point EULAR/ACR presentation associated with tendonitis.
Following initiation of HRT, joint symptoms improved within two months, indicating that the condition had not yet progressed to RA. Consequently, MTX and biologic agents were ineffective at this stage. The first two treating physicians diagnosed RA and primarily administered MTX. Although RF and anti-CCP antibody levels decreased, the patient’s joint symptoms persisted. The second physician discontinued MTX in July 2023 due to adverse effects and pursued alternative therapies; RF levels continued to rise, yet CRP remained below 0.03 mg/dL, and no active inflammation was observed.
Upon evaluation by the third physician in December 2024, RA was questioned based on hand radiographs and palpation findings. The patient was diagnosed with menopausal arthritis, tendonitis, and osteoarthritis, and HRT was initiated. This intervention led to improvements in daily activity and general fatigue. On February 22, 2025, the patient developed swelling and redness in her joints with a concurrent CRP rise to 1.99 mg/dL, confirming the onset of RA. HRT was continued alongside MTX 12 mg weekly and subcutaneous ETN 25 mg/w, which achieved complete remission within three months. Notably, prior treatments had only affected tendon sheaths and were ineffective against synovial lesions of RA. This suggests that early HRT might have delayed or prevented the onset of RA (8), potentially reducing the need for MTX or biologics, which had been ineffective since January 2022. Finally, hand XP revealed no evidence of bone erosion both first visit in December 2024 and latest visit in September 2025.
A limitation of this case is that the patient’s self-reported joint pain cannot be attributed solely to estrogen deficiency. Environmental factors, particularly seasonal changes, and psychosocial stressors, including challenges at home and in the workplace, likely contributed to symptom fluctuations.
ACKNOWLEDGEMENT
We thank Dr. S. Inokuma for her valuable suggestions on this manuscript.
FUNDING
None
CONFLICT OF INTEREST
None
- Malgorzata Magliano Menopausal arthralgia: Fact or fiction. Maturitas 2010 Sep;67(1):29-33. doi: 10.1016/j.maturitas.2010.04.009.
- Burkard T, Rauch M, Spoendlin J, Prieto-Alhambra D, Jick SS, Meier CR. Risk of hand osteoarthritis in new users of hormone replacement therapy: A nested case-control analysis. Maturitas. 2020 Feb; 132: 17-23. doi: 10.1016/j.maturitas.2019.11.006. Epub 2019 Nov 27. PMID: 31883658.
- Pang H, Chen S, Klyne DM, Harrich D, Ding W, Yang S, Han FY. Low back pain and osteoarthritis pain: a perspective of estrogen. Bone Res. 2023 Aug 4;11(1):42. doi: 10.1038/s41413-023-00280-x. PMID: 37542028; PMCID: PMC10403578.
- Jung JH, Bang CH, Song GG, Kim C, Kim JH, Choi SJ. Knee osteoarthritis and menopausal hormone therapy in postmenopausal women: a nationwide cross-sectional study. Menopause. 2018 Dec 21;26(6):598-602. doi: 10.1097/GME.0000000000001280. PMID: 30586007.10.1016/j.joca.2022.07.010. Epub 2022 Aug 19. PMID: 35995128.
- Amano T, Imao T, Takemae K. Clinical efficacy of Japanese traditional herbal medicine (Kampo) in patients with late-onset hypogonadism. Aging Male. 2010 Sep;13(3):166-73. doi: 10.3109/13685530903536684.PMID: 20143961
- Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62(9): 2569-2581, 2010
- Gomez D, Saavedra-Martinez G, Villarreal L et al. Misdiagnosis of rheumatoid arthritis-The photography. Ann Rheuma Dis 2015;74 Suppl 2: 689.
- Cecilia Orellana,Saedis Saevarsdottir, Lars Klareskog, Elizabeth W Karlson, Lars Alfredsson, Camilla Bengtsson. Postmenopausal hormone therapy and the risk of rheumatoid arthritis: results from the Swedish EIRA population-based case-control study Eur J Epidemiol. 2015 May;30(5):449-57. doi: 10.1007/s10654-015-0004-y. Epub 2015 Mar 12
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- BioMed Research Journal (ISSN:2578-8892)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Pathology and Toxicology Research
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)


