
93
Views & Citations10
Likes & Shares
Result: The overall prevalence of contraceptive “ever use” was 85.5% while that of “current use” was 50.0%. Factors that were significantly associated with use include: [ Ever use, age (P=0.004), marital status (P=0.000), no. of children (P=0.002) ; Current use age ( P= 0.022), marital status, (P= 0.009) and number of children (P=0.001)] Logistic regression analysis indicated that age greater than 35 years was a significant predictor of ever use ( O.R= 2.91. CI - 1.10-7.66) while having 3 or more children was the most important predictor of current use (O.R = 3.63, 95% CI = 1.16-11.74).
Conclusion: Modern contraceptive utilization among the female health care workers in this study was higher than Nigerian estimates for women in the general population. Though the personal choices of the health workers may not directly affect patients care, their perspectives and experiences can improve and inform the provision of reproductive health care and services.
Keywords: Modern contraceptives, Healthcare workers, Determinants, Utilization.
The front-liners responsible for providing family planning services are the health workers. Their responsibility includes giving clients accurate and thorough information about family planning and by so doing assist them make informed decisions about the choice of family planning method they desire [11]. Nevertheless, personal biases can hinder health workers ability to amply assess the needs of clients and as such create barriers to client’s choice [12]. Health workers that provide family planning counselling include physicians from different specialties (Obstetrics and gynaecology, family medicine, paediatrics, emergency medicine, nursing services, physician assistance, community health workers, pharmacy, among others [13]. These health workers are drawn from diverse educational backgrounds resulting in different comfort and competence levels in provision of contraceptive services. Studies have shown that there is health workers bias regarding specific modern contraceptives and their utilization in some populations. The contraceptive counselling practices of health workers may be affected by their understanding of the medical eligibility for some certain group, perception of the pregnancy risk, prior medical training and the setting of the workplace [14,15,16]. Health workers ethnic and racial biases may impact their discussions with women desirous of contraception [17,18]. Evidence of bias based on parity, age of client and marital status among other parameters has been documented; the commonest of the health worker bias reported was that against providing various types of methods of contraception to the youth [12]. While many family planning seekers desire a valuable contribution and ideas from their health care providers and would want a comprehensive and detailed information regarding their choices of contraception, many clients still desire their autonomy in choosing their method of contraception [11]
In Germany, about 37.2% of the female obstetricians and gynaecologist reported use of combined oral contraceptives personally [19]. In Spain, a study compared contraceptive use among female health workers and other females in the general population and it was noted that condoms were the preferred method in both groups due to fear of side effects. However, the female health care workers chose long-acting methods that are reversible compared to oral contraceptive pills preferred by the females in the general population [20]
A study done in Ghana among health workers and medical student in clinical classes on the attitude and practice of contraception showed that greater than half of the respondents (62.4%) used a type of contraceptive while only 18% were using it as the time of the study and barrier methods and condom were preferable [21]. In Nigeria a cross-sectional study that sought to know the attitude of health care workers regarding the provision of contraception to adolescents showed that many of the health care workers (57.7%) had an unfavourable attitude towards offering contraception to adolescents [22].
The front-line workers in delivering and advocating for modern contraception are the health care workers and there is the possibility that clients may ask for the health workers experiences if they had used or are using a particular method [23]
The front-line workers in delivering and advocating for modern contraception are the health care workers and there is the possibility that clients may ask for the health workers’ experiences if they had used or are using a particular method. Are the health care workers living by example by utilizing modern contraceptives and what are the factors that influence their use? It is therefore very pertinent to understand the feelings of health workers about the various methods of contraception and how their views may affect their interactions with the clients and finally their client’s chosen method. We therefore sought to determine the prevalence, pattern and the factors that determine the choice of modern contraction among female health care workers in tertiary centre in south east Nigeria.
MATERIALS AND METHOD
Study design/Setting:
This was a cross-sectional study. This study was conducted between March to September 2024 at the various clinics of Enugu State University of Science & Technology (ESUT) Teaching Hospital, Parklane. The hospital, located in Enugu which is one of the states in the south Eastern part of Nigeria. It is a state-owned teaching hospital located at the city centre with different cadres and specialties of health workers working in it. The hospital receives referral from the surrounding areas like the south east, south-south and the north central regions of the country and thus has a high inflow of patients and clients. This hospital is a public hospital that offers free maternal care. It has a family planning unit that provides a wide range of modern contraceptive methods. These methods include: injectables, implants, intrauterine contraceptive (IUCD), combined oral contraception, condoms (male and female), emergency contraceptive pills and sterilization (tubal ligation) methods. It has a population of over 700 female healthcare workers
Sampling Population: This study was conducted among professional female health care workers at the Enugu State University of Science & Technology (ESUT) Teaching Hospital, Parklane. Professional health care workers were those who underwent formal training in a professional health course with a minimum professional certification.
Sample size/Sampling approach
The sample size of 217 participants was obtained by using Fisher’s formula for cross sectional studies [24] and at 5% error limit. Using a modern contraceptive prevalence rate of 15% [9]. First the entire health services department at the hospital was identified and the number of all female health care workers in each department was obtained (which includes the Obstetrics and gynaecology as well as the family planning unit, general outpatient, surgery, paediatrics, internal medicine, emergency departments). Consecutive sampling technique was used in selecting qualified participants.
Inclusion and Exclusion Criteria
Only the female professional health workers were included. Non-professional female health care workers like the cleaners, drivers, record keepers, security guards as well as male healthcare workers were excluded.
Ethical Considerations
Ethical approval was obtained from the Ethical Review Committee of the Enugu State University of Science and Technology Teaching Hospital, Parklane with ethical clearance certificate no. ESUTHP/C-MAC/RA/034/Vol.4/25. Written consent was obtained from the respondents prior to participation. Participation was voluntary and written informed consent was obtained. Participants were very free to withdraw from the study at any point in time during the study. Respect for persons, beneficence and justice were ensured. The data was also securely stored to ensure confidentiality of information.
Data collection and Management
A pretested, self-administered questionnaire was used for collection of data. The questionnaire was structured with a mix of close and open-ended questions and was specially designed and prepared to compile information relating to the objectives of the study. The questionnaires were pretested using 10% of the sample size in the department and the required corrections were made before the main study. Four research assistants (females) were employed and trained in data collection. Participants were given explanations about the nature of the study after which a written informed consent was obtained prior to participation. Participants were recruited using the convenient consecutive technique till the sample size was achieved. Information on demographic characteristics, reproductive and sexual history as well as modern contraceptives were obtained from the participants.
Data Analysis
The questionnaires were cleaned and checked for completeness, coded and entered in the Statistical Package for Social Sciences version 25 and analysis done. The independent variables include the Socio-demographic characteristics such as age, religion, level of education, marital status, place of residence, number of children etc. The dependent variable was the use of modern contraceptives. The demographic variables and descriptive statistics were reported in frequencies and percentages (Uni-variate analysis). Associations between the dependent variable (modern contraceptive use) and the socio demographic characteristic were also analysed to determine significant association using chi square testing. In order to determine the significant predictors of modern contraceptive use, a multivariate analysis (logistic regression) was also done. The level of significance of all associations was set at 0.05%.
Result
Descriptive Statistics
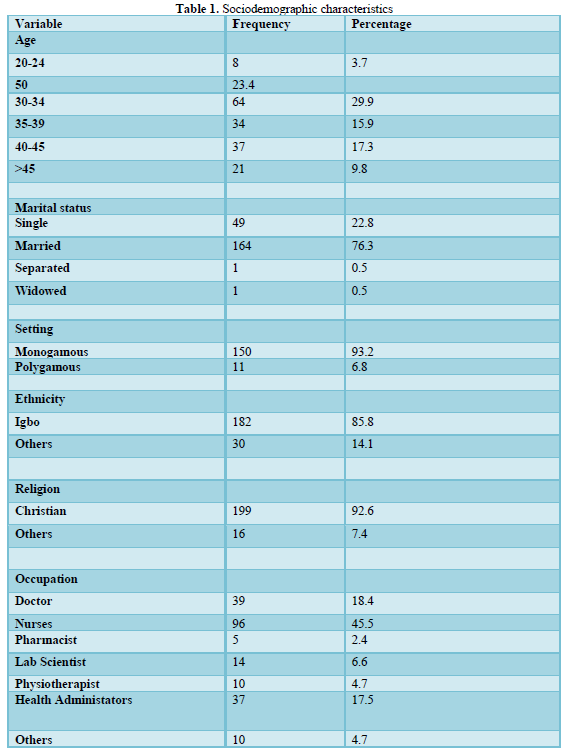
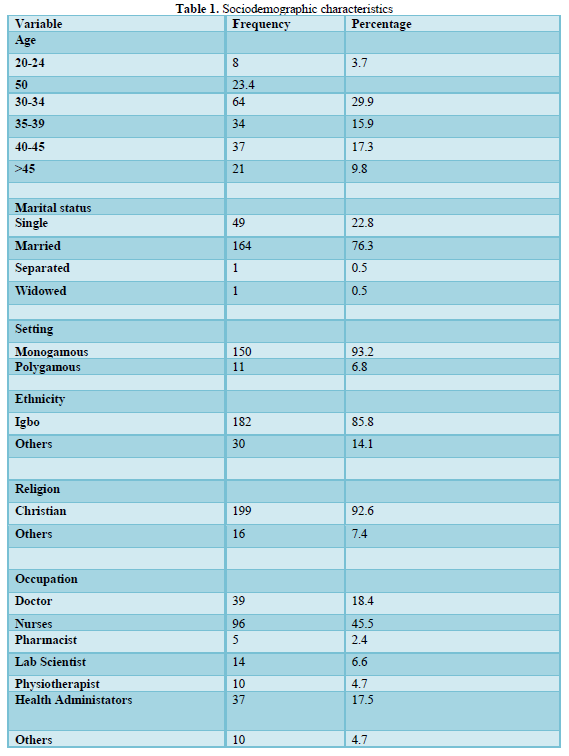
Two hundred and seventeen women were studied. (Table 1) shows the frequency distribution of respondents’ characteristics. The age group 30-34 years had the highest number of women (29.9%) while the group 20- 24 years had the lowest (3.7%). They were mostly married women (76.3%). Among married respondents, the majority of them (93.2%) were in monogamous union. The respondents were mainly nurses (45.5%). Others include the doctors, pharmacists, physiotherapists etc.
Obstetrics Characteristics of Participants
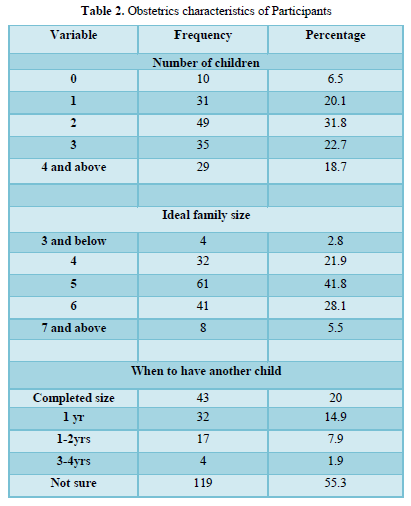
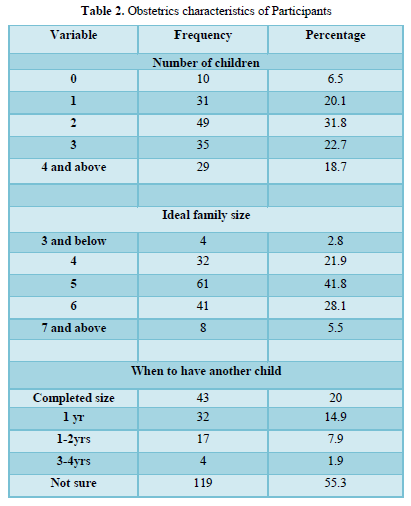
About a third of the women (31.8%) had 2 children, while 6.5% had none (Table 2). The ideal family size reported most was five (41.8%), while those who wanted a family size of 3 and below were few (2,8%). Concerning when the participant wanted to have another child, more than half (55.3%) did not know when but about 15% of the women were ready to have more children within one year.
Prevalence and method choice
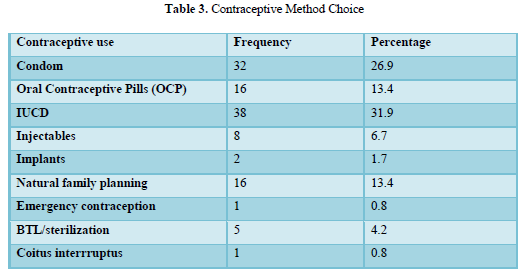
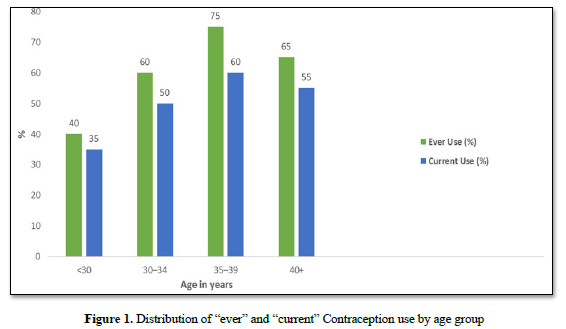
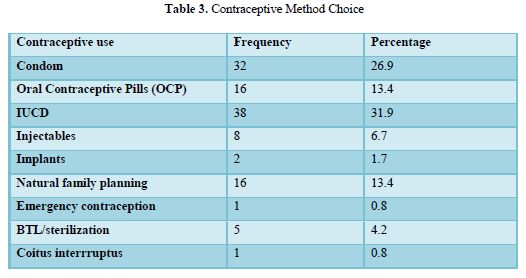
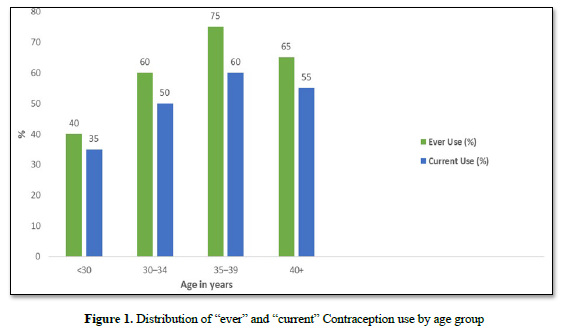
The overall prevalence of contraceptive use (ever use) was 85.5% while that of current contraceptive use was 50.0%. The age group 35 - 39 years had the highest use of contraception with ‘ever use’ and ‘current use’ of 70% and 65% respectively. Contraceptive use continued to increase till age 40 years and above when it showed a decline (Figure 1). The most common contraceptive method used by the women was intrauterine device (31.9%).
Bivariate analysis
Relationship between ever use of contraceptive and women’s characteristics
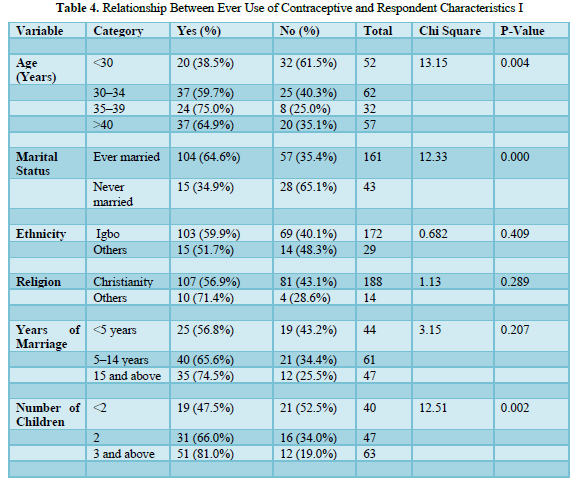
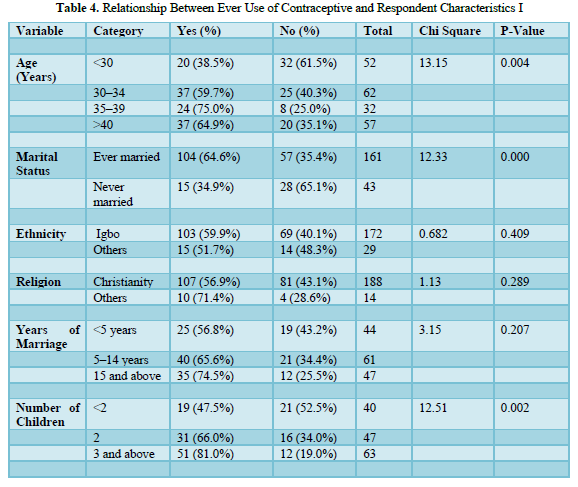
Table 5 shows the relationship between ever use of contraceptives and respondents’ characteristics. Significant results were found for age (p=0.004), marital status (p<0.001), number of children (p=0.002), Specifically contraceptive use increased with age with 38.5% of those aged less than 30 years compared with 59.7% of those 30-34 years, 75% of the 35–39-year age group and 64.9% of those 40 years and above (Figure 5). Women who had ever married or in marital unions at time of interview reported higher contraceptive use (64.6%) compared to those who never married (34.9%). The proportion of respondents who ever used contraceptives also increased with the number of children. For those with less than two children, 47.5% had used a contraceptive compared to 65.6% of those with two children and 81% of those with 3 or more children. There were no significant relationships for ethnicity, religion and years of marriage even though use increased with years of marriage.
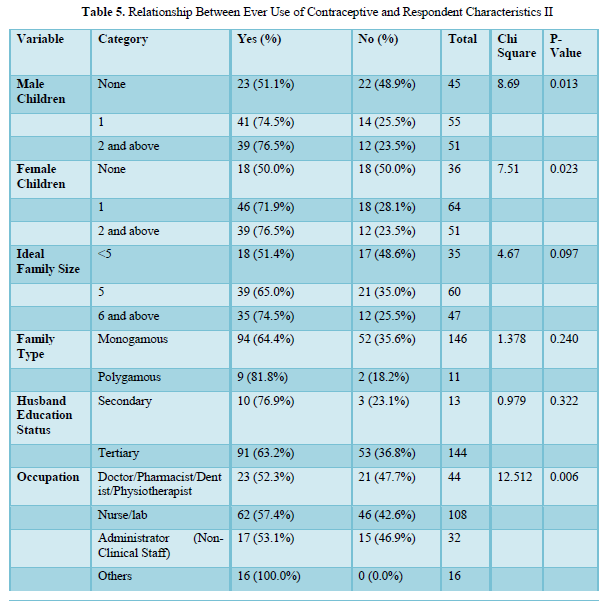
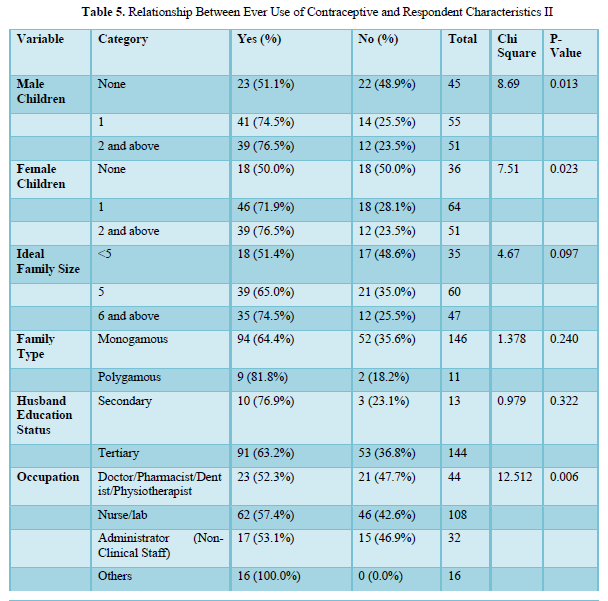
There is also a significant association between ever use and number of male children (p=0.013), female children (p=0.023) and occupation (p=0.006) (Table 6) The proportion increased with increased number of male and female children. Concerning occupational groups, 52.3% of doctors, pharmacists, dentists and physiotherapists had used contraceptive compared to 57.4% of nurses or laboratory scientists, 53.1% of non-clinical staff and all of the other professions. Women’s choice of ideal family size, type of marriage and husband’s education were not significantly related.
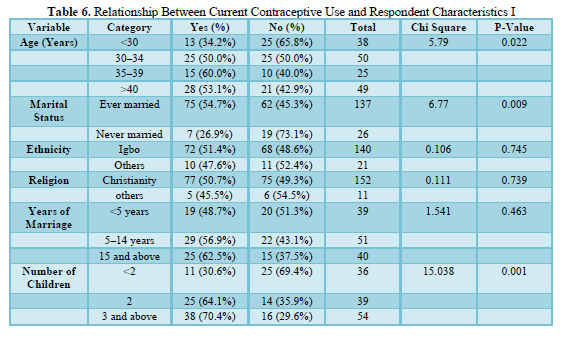
Relationship between current contraceptive use and women’s characteristics
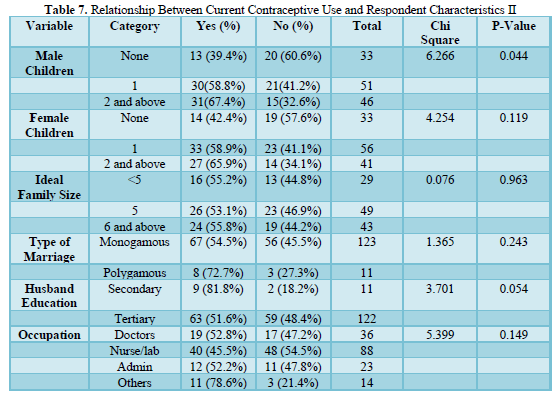
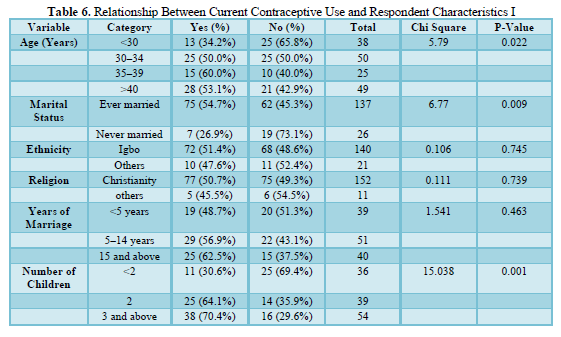
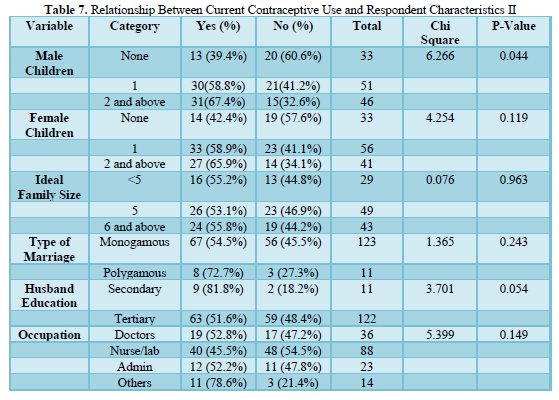
Concerning current use, significant relationships were found for marital status (p=0.009), number of children (p=0.001) and male children (p=0.044). Women who ever married reported higher contraceptive usage (54.7%) compared to those who never married (26.9%). The proportion currently using contraceptives increased with the number of children, 30.6% for women with less than two children, 64.1% for those with two children and 70.4% for those with three or more children. Over a third of those with no male child compared to 58.8% of those with one child and 67.4% of those with two or more children were current contraceptive users. Other variables were not significant.
Multi Variate Analysis
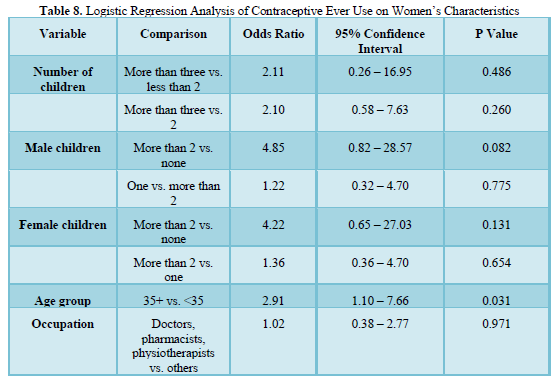
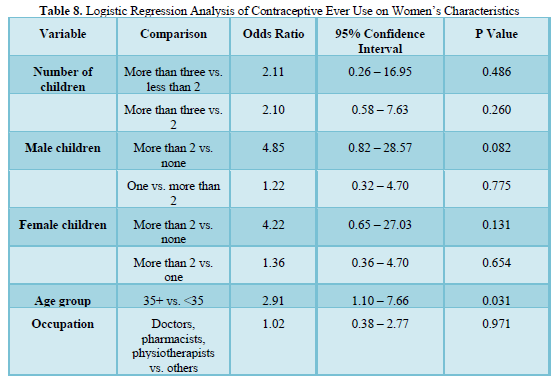
Logistic regression analysis was carried out to identify significant variables after adjusting for con-founders. (Table 8) shows the results from the regression analysis. Significant results were gotten for age. Those greater than 35years were about three times more likely to have used contraceptives (95% CI OR =1.10 -7.65). Other variables such as number of children and number of male and female children were not significant on logistic regression.
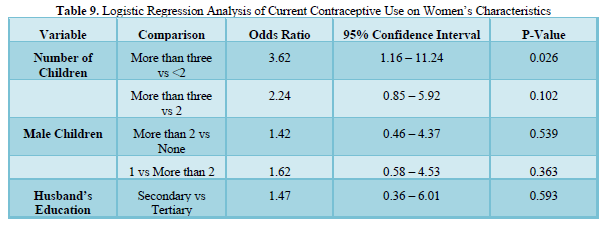
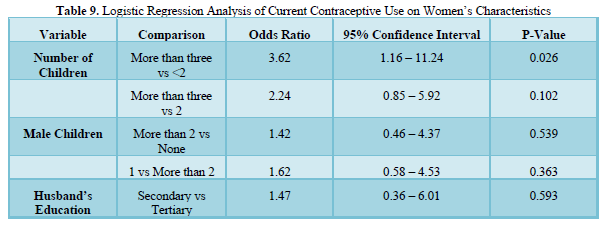
(Table 9) shows the results from the logistic regression analysis on current use. Significant results were obtained for the number of children. Those with three or more children were about 3.6 times more likely than those with less than 2 children to be current users (95% CI OR =1.16 – 11.24). The husband’s education and number of male children were not significant.
DISCUSSION
This study aimed to determine the prevalence, pattern and determinants of modern contraceptive use among the female health workers at a tertiary health facility. The overall prevalence of contraceptive use (ever use) was 85.5% while that of current contraceptive use was 50.0%. This was similar to the findings of studies done among health care workers in Ile Ife [25], Uganda [26]. Malaysia [27] where it was noted the prevalence of modern contraceptives were 75.2%, 75%, and 82% respectively. In this study also, the prevalence of current contraceptive use was 50% and this is comparable to the finding in Ife where the prevalence was about 57%. However, these findings are significantly higher than the prevalence of modern contraceptives in the general population in Nigeria where the prevalence of modern contraceptive use is 15% [9]. Again, there is a significantly lower prevalence according to a study among rural women in the general population of in south west Nigeria [28]. The higher prevalence noted in these studies among health workers compared to the general population may be due to the better knowledge and access. Health care workers due to their profession are more likely to know the risks and benefits of contraception and may also have a better access to contraceptive resources including counselling, education as well as family planning methods. Health workers’ professional insight may enable them to have an in-depth understanding of the importance of contraception in preventing unwanted pregnancy and in reducing infant and maternal mortality. Health care workers may also feel more professionally and personally empowered in making decisions concerning their reproductive health. They may also prioritize contraception as a method to model good healthy behaviour from their community and patients. Female health care workers who utilize contraceptives could serve as influencers and role models promoting education and awareness about family planning and reproductive health among their communities and patients. By utilizing modern contraceptives, the female health care workers are more likely to advocate for programmes and policies that support family planning and reproductive health, potentially influencing leadership and health policy.
In the study, the most commonly used modern method among the female health workers was intrauterine contraceptives with about one third of the participants (31.9%) preferring the method. This finding is similar to that found in Uganda and in Ghana where the barrier method was the preferred method [21,26], however this is in contrast with a study done with female health workers in Spain and in their general population where it was noted that condom was the most preferred method [20]. In Nigeria and among the general population, the commonly used methods among the married women were implants and injectables [9]. Again, cross-sectional studies across the sub-Saharan African nations also noted that implants (26.5%) and injectables (39.4%) were the most commonly preferred modern contraceptives among married women in the general population [29]. A larger population survey among 20 African nations noted a similar finding [30]. The observed difference in method choice among females in the general population and the female health workers may be attributed to the fact that the health professionals have more knowledge than the women in the general population about the side effects of the barrier methods compared to the hormonal method [31], that the barrier methods can be stopped at any time without compromising the hormonal cycle of the their body with resultant instantaneous resumption of fertility, as well as the ease of use of the barrier methods [20].
Bi-variate analysis showed that factors that determine the use of modern contraceptive methods among female health care workers include age, marital status, and number of children. This resonates with national trends. Studies done in Nigeria similarly showed that marital status and age are crucial determinants of use of modern contraceptive methods [32,33]. This emphasizes the need for a nuanced intervention that targets specific marital cohorts and age groups. Although significant variations occur across nations on how different factors; community, individual and service delivery influence use of modern contraceptive methods. Many of the factors are conformable across nations with the findings in many studies done across Africa [34, 35, 36, and other countries of the world [37,38].
At the multivariate analysis for ever and current use of modern contraceptive significant predictors included age and number of living children respectively. Those greater than 35 years were about three times more likely to have used contraceptives. Again, those with 3 or more children were about 3.6 times more likely than those with less than 2 children to be current users. A study in Ghana which sought to describe the use of highly effective contraceptives by parity also showed that a woman's age as well as the number of living children are among the predictors of modern contraceptive use [39]. It was also noted that the women with one child or no child are not likely or less likely to utilize modern contraception probably because they do see the need for use of contraceptives at that time or due to their desire for more children [40]. In contrast, women with up to four children or more are likely to utilize contraceptives and prevent unwanted or unintended pregnancies having completed their family size.
The limitations of this study include the fact that this was a cross-sectional study which obviates the ability of making causal inferences. The individual staff may have reported what is desired or expected of them instead of the reality and as such lead to “desirability bias”, however questions were designed to limit this as much as it was possible. Again, due to a busy work schedule, the staff would have given hasty responses. This was limited by ensuring that each participant was also allowed to choose the appropriate time for their interviews.
CONCLUSION
The prevalence of “ever use” and “current use” of modern contraceptives among the female health care workers in this study is higher than the Nigerian estimate for women in the general population. The commonest method used was intrauterine contraceptive devices. Maternal age and number of living children were the most important determinants of use. Though the personal choices of the health workers may not directly affect patients’ care, their perspectives and experiences can improve and inform the provision of reproductive health care and services.
- Gold RB (2005) The implications of defining when a woman is pregnant. The Guttmacher report on public policy” 8(2):7-10.
- Trends in contraceptive use worldwide (2015). Department of Economic and Social Affairs, Population Division Newyork.
- Li Q, Rimon JG (2018) A demographic dividend of the FP2020 Initiative and the SDG reproductive health target: Case studies of India and Nigeria. Gates Open Research;12.
- Kennedy CE, Yeh PT, Gaffield ME (2020) Contraception values and preferences: protocol and methods for a global systematic review. Contraception 101(2):69–73.
- Yeh PT, Kautsar H, Kennedy CE, Gaffield ME (2022) Values and preferences for contraception: A global systematic review. Contraception 111:3–21.
- Wulifan JK, Brenner S, Jahn A, De Allegri M (2016) A scoping review on determinants of unmet need for family planning among women of reproductive age in low and middle income countries. BMC Womens Health 16(1):2.
- Ewerling F, Victora CG, Raj A, Coll C, Hellwig F et al (2018). Demand for familyplanning satisfied with modern methods among sexually active women in low-and middle-income countries: who is lagging behind? Reprod Health. 15(1):1–10.
- Kantorová V, Wheldon MC, Ueffing P, Dasgupta ANZ (2020) Estimating progress towards meeting women’s contraceptive needs in 185 countries: A Bayesian hierarchical modelling study. PLoS Med 17(2):e1003026.
- Federal Ministry of Health and Social Welfare of Nigeria (2024) National Population Commission (NPC) [Nigeria], and ICF. Nigeria Demographic and Health Survey. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF;
- Abubarkar IB (2021) Correlates of Modern Contraceptive Use Among Nigerian Women: Evidence from Nigerian Demographic Health Survey 2018 Poster abstracts. Int J Gynaecol Obstet 155(S2):127–532.
- Komal S, Soina, Yeha PT, Gaffieldc ME, Ge D C (2022) Health workers’ values and preferences regarding contraceptive methods globally: A systematic review.111:61–70.
- Solo J, Festin M. (2019) Provider bias in family planning services: A review of its meaning and manifestations. Glob Health Sci Pract [Internet]. 7(3):371–85.
- Coulter I, Jacobson P, Parker LE(2000) Sharing the mantle of primary female care: physicians, nurse practitioners, and physician assistants. J Am Med Womens Assoc. Spring;55(2):100–103.
- Akers AY, Gold MA, Borrero S. Santucci AScHealth et al (2010). Providers’ perspectives on challenges to contraceptive counseling in primary care settings. J Womens Health (Larchmt)19: 1163–1170.
- Wang Z, Yuan W, Tu X, Liang H, Miao M, et al, (2020) Misconceptions and beliefs regarding the use of intrauterine devices for nulliparous women among Chinese health care providers. J Pediatr Adolesc Gynecol 33(1):33–38.
- Hopkins B (2017) Barriers to health care providers’ provision of long-acting reversible contraception to adolescent and nulliparous young women. Nurs Women’s. Health. 21:122–8.
- Dehlendorf C, Levy K, Kelley A, Grumbach K, Steinauer J (2013) Women’s preferences for contraceptive counseling and decision making. Contraception 88(2):250–256.
- Finer LB, Zolna MR (2011) Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 84(5):478–485.
- Wiegratz I, Galiläer K, Sänger N, Rody A, Kuhl H, et al (2010). Prescribing preferences and personal experience of female gynaecologists in Germany and Austria regarding use of extended-cycle oral contraceptives. Eur J Contracept Reprod Health Care 15(6):405–412.
- Lete I, Pérez-Campos E (2014) Differences in contraceptive use between Spanish female healthcare providers and Spanish women in the general population aged 23 to 49 years: the HABITS Study. Eur J Contracept Reprod Health Care 19(3):161–168.
- Agbeno EK, Osarfo J, Anane-Fenin B, Achampong EK, Neequaye NA, et al (2021) Attitudes and practices of healthcare professionals and clinical medical students on contraception: A cross-sectional study in cape coast, Ghana. Int J Reprod Med :6631790.
- Ahanonu EL (2014) Attitudes of Healthcare Providers towards Providing Contraceptives for Unmarried Adolescents in Ibadan, Nigeria. J Family Reprod Health. 8:33–40.
- Manu A, Arifeen S, Williams J, Mwasanya E, Zaka N, et al (2018). Assessment of facility readiness for implementing the WHO/UNICEF standards for improving quality of maternal and newborn care in health facilities – experiences from UNICEF’s implementation in three countries of South Asia and sub-Saharan Africa. BMC Health Serv Res 18(1).
- Chen M (2004)Sample size determination: the fundamentals of international clinical research workshop. Family Health International. 1–18.
- Olaleye A, Orji E, Akintayo A, Olaleye A, Imaralu J (2015) Perception and uptake of contraception among health workers in Ile-Ife, South-western Nigeria. Babcock University Medical Journal (BUMJ) 1(1):21–28.
- Opiro K, Opee J, Sikoti M, Pebalo PF, Ayikoru JH, (2024) et al. Utilization of modern contraceptives among female health care workers at Gulu university teaching hospitals in Northern Uganda. Contracept Reprod Med 9(1):13.
- Suhaimi H, Monga D, Siva A. (1996) A study of Knowledge and Attitude towards contraception among healthcare staff in Kelantan (Malaysia). Singapore Med J. 1996;36:51–54.
- Orji EO, Onwudiegwu U (2022) Prevalence and determinants of contraceptive practice in a defined Nigerian population. J Obstet Gynaecol 22(5):540–543.
- Boadu I (2022) Coverage and determinants of modern contraceptive use in sub Saharan Africa: further analysis of demographic and health surveys. Reprod Health. 19(1).
- Apanga PA, Kumbeni MT, Ayamga EA, Ulanja MB, Akparibo R (2020) Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: a large population-based study. BMJ Open 10(9):e041103.
- Kibira SPS, Muhumuza C, Bukenya JN, Atuyambe LM.(2015) “I spent a full month bleeding, I thought I was going to die…” A qualitative study of experiences of women using modern contraception in Wakiso district, Uganda. PLoS One 10(11):e0141998.
- Durowade KA, Omokanye LO, Elegbede OE, Adetokunbo S, Olomofe CO, (2017) et al. Barriers to contraceptive uptake among women of reproductive age in a semi-urban community of Ekiti State, Southwest Nigeria. Ethiop J Health Sci 27(2):121–128.
- Abubakar IB, Abubakar HB (2024) Nigerian women’s modern contraceptive use: Evidence from NDHS 2018. Reprod Fertil. 5(2).
- Blackstone SR, Nwaozuru U, Iwelunmor J (2017) Factors influencing contraceptive use in sub-Saharan Africa: A systematic review. Int Q Community Health Educ [Internet]. 37(2):79–91.
- Okoeguale J, Osagiede EF, Idumwonyi O, Ehigiegba AE (2022). Factors influencing the use of modern contraceptives amongst postpartum women in a rural tertiary hospital in South-South Nigeria. ajol.info 26(1).
- Afriyie P, Tarkang EE (2019) Factors influencing use of modern contraception among married women in Ho West district, Ghana: descriptive cross-sectional study. Pan Afr Med J [Internet]. 2019;33:15.
- Kistiana S, Gayatri M, Sari DP (2020) Determinants of modern contraceptive use among young married women (age 15-24) in Indonesia. Glob J Health Sci 12(13):37.
- Subedi R, Jahan I, Baatsen P (2018) Factors influencing modern contraceptive use among adolescents in Nepal. J Nepal Health Res Counc 16(3):251–256.
- Compton S, Nakua E, Moyer C, Dzomeku V, Treleaven E, et al (2023). Contraceptive use by number of living children in Ghana: Evidence from the 2017 maternal health survey. PLoS One 18(12):e0295815.
- Teshale AB, Wang VQ, Biney GK, Ameyaw EK, Adjei NK, et al (2023). Contraceptive use pattern based on the number and composition of children among married women in sub-Saharan Africa: a multilevel analysis. Contracept Reprod Med 8(1).
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Rheumatology Research (ISSN:2641-6999)


