277
Views & Citations10
Likes & Shares
Infant Welfare Card (IWC) was available to 287 (95.7%) with 74.6% fully immunized before 12 months and 80.5% fully immunized by 24 months. Partially immunized account for 56 (19.5%) with 13 (23.2%) being unaware of the need to return for a second or third dose; 11 (19.6%) the place and/or time of immunization was unknown; 12 (21.4%) too busy while 6 (10.7%) unaware of the need for immunization.
Infectious illnesses are the main cause of morbidity and death in children, and immunization is crucial for their health. In the Gambia, 95.7% of children aged 12-23 months had an Infant Welfare Card, with 74.6% fully immunized by 12 months and 80.5% by 24 months. The immunization rate in the Gambia needs increased coverage and better practices.
Keywords: Immunization, Coverage survey, Fully immunized, Partially immunized, Dropout rate
Global coverage of immunization was 86% in 2019 but dropped to 83% in 2020. In 2009, approximately 23 million children under one year of age did not receive basic vaccines, and the number of completely unvaccinated children increased by 2.3 million in 2020. The Expanded Programme of Immunization (EPI) was initiated by the World Health Organization in 1974 to immunize children against six deadly diseases: childhood tuberculosis, Hepatitis B, Measles, Poliomyelitis, Diphtheria, Pertussis, and Tetanus [4]. The Gambia has added Hemophilus influenza type b to the EPI, currently as pentavalent diphtheria-tetanus-pertussis-Hib-hep B vaccine.
The national Expanded Programme on Immunization (EPI) was launched as part of the Primary Health Care (PHC) strategy in 1979/80. The main strengths of the EPI are high accessibility with 85% geographical coverage, high coverage rates reaching over 80% for most antigens; high public awareness and demand for immunization, and the near eradication of poliomyelitis.
Since its inception in May 1979, the EPI has progressively increased immunization coverage within its target population to its present coverage of 80% of fully immunized children less than one year of age. Initially, the program used the mobile strategy (i.e. visiting villages and immunizing target children and pregnant women), which was found to be expensive and would not be sustained. In that regard, the Department of State for Health and Social Welfare (DOSH) decided to use the Maternal and Child Health (MCH) teams to deliver immunization services at all the static and outreach immunization sites. In 1995 the DOSH decided to involve the private clinics in the provision of immunization services to increase immunization delivery points.
A look at the infant mortality rate (IMR) of developed as well as developing/transitional countries (including The Gambia), shows an increased incidence of mortality and morbidity among children globally [5,6]. Therefore, increasing the general population’s access to immunization services may reduce IMR at large [7]. However, to meet the goal of increased immunization coverage, barriers to immunization should be identified and addressed [8]. A decrease in multiple VPD has been noticed for multiple years [9], with an increase in the number of unvaccinated children reported recently.
In the Gambia, more 85% of immunization coverage is registered for individual vaccine doses [10]. The success could be attributed to good access to immunizations through the reproductive and child health (RCH) clinics. Importantly, vaccines are offered free of charge at all immunization points regardless of whether a government or nongovernment health facility runs the immunization service point. Despite the registered successes in immunization, there exist disparities between rural (83.8%) and urban (67.7%) immunization coverage [11], which could be attributed to several factors in the urban areas. Previous studies have investigated immunization coverage, timeliness, cost-effectiveness, and the impact of selected vaccines in many countries, including The Gambia [12] (Tables 1-3).
According to World Health Organization data, by 2011, there were 83%, 84%, and 84% of people worldwide who had had three doses of DTP, one dose of measles vaccination, and three doses of polio vaccine, respectively. However, more than one-fifth of children worldwide, particularly those in low-income nations, were still at risk for vaccine-preventable morbidity and death at the age of 12 months because they had not received all of their recommended vaccinations [13].
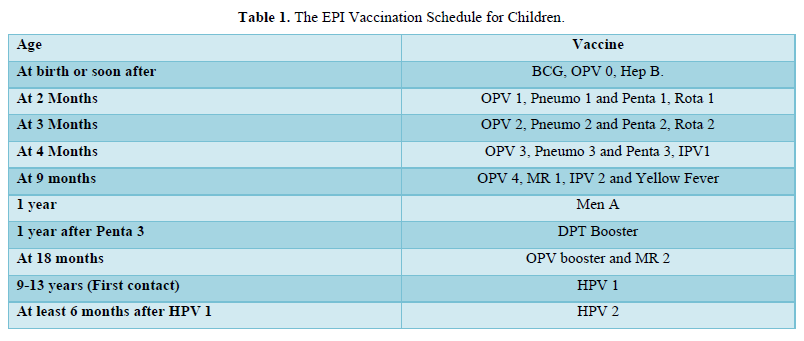
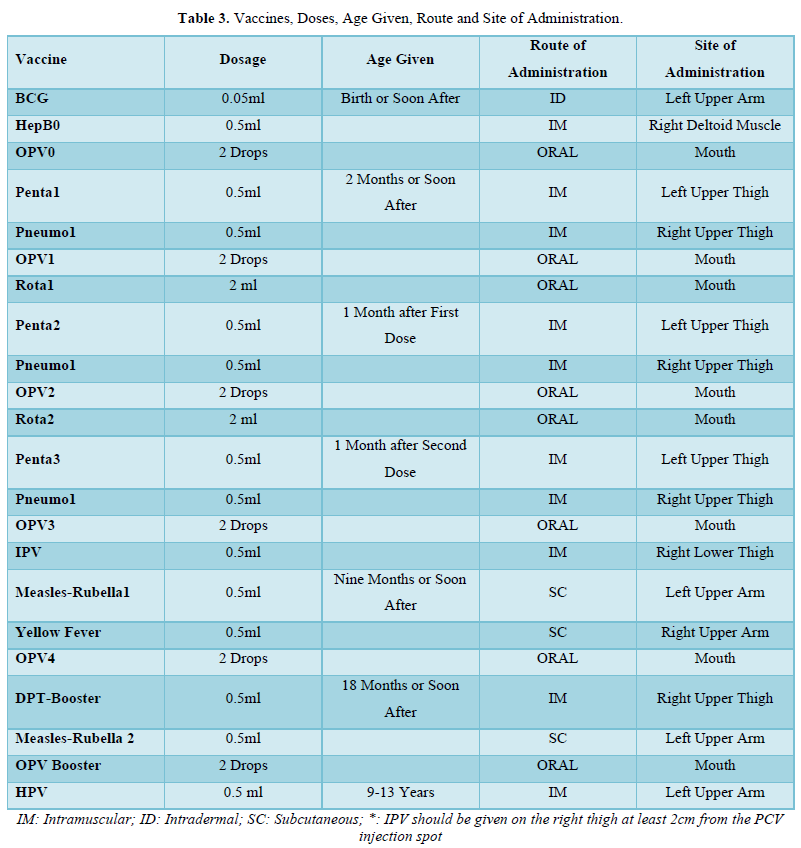
In The Gambia, the immunization policy calls for BCG vaccine given at birth or at first contact, three doses of pentavalent (DPT-HepB-Hib) vaccine and the newly added pneumococcal conjugate vaccine (PCV) vaccine given at approximately 4, 8, and 12 weeks of age, four doses of oral polio vaccine given approximately at 0-2, 4, 8, and 12 weeks of age, and measles vaccine given at or soon after reaching 9 months of age [14]. Within a year of a child's age, it is advised that they receive all of these vaccinations [14].
Three-fourths (76%) of the children polled had at least one vaccination, and 36% had received all recommended vaccinations, according to research on immunization coverage of children aged 12 to 23 months that was conducted in Jigjiga district of the Somali National Regional State of Ethiopia. BCG (41.8%), OPV3 (27.5%), and Measles (24.9%) coverage per antigen [15]. Another study by Martin Nyaaba Adokiya et al, 2016, revealed that out of 600 children surveyed, 89,5% were fully immunized while 9.5% were partially immunized while 1.0% had not received any vaccine [16]. In the same study, it has revealed that of the 63 children not fully immunized, 57.1% reported time was not convenient and 14.3% said the place of immunization was not known or the mother was too busy.
Another study conducted by Elias legesse and Worku Dechasi in 2013 assessing child immunization coverage and its determination in Sinana district, Southeast Ethiopia revealed that 76.8% of Children aged 12 to 23 months were fully vaccinated by card plus history while 85.4% had OPV3 and 77.7% had Measles, and 84.6% had Penta3 [17].
A cross-sectional survey was conducted in Dechang, West Region Cameroun during a polio outbreak on vaccine coverage and determinants in incomplete vaccination in children aged 12 - 23 months revealing that 85.9% of the children were fully immunized while 14.1% were partially immunized. Out of those partially immunized the reason was mothers too busy accounted for 32.2% (n=22). 98.8% had Measles; 92.8% Penta3; 91.6% OPV3; 90% Measles; 90% yellow fever; partially immunized 15.5%; fully immunized less than or equal to 24 months 84.5% and fully immunized by 12 months of age 73.4% [18].
Despite all the efforts the governmental and non‑governmental institutes put in for 100% immunization coverage, there are still pockets of low coverage areas [13]. The Gambia Expanded Programme on Immunization services are offered free in public health facilities private clinics and Hospitals, but despite rapid increases, the immunization rate remains low in some areas.
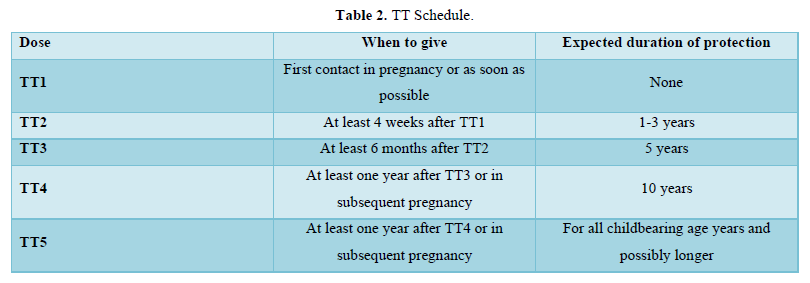
The focus is on providing routine vaccination using mobile teams for traditional EPI antigens (BCG, DPT, Oral Polio Vaccine, Measles), Tetanus Toxoid vaccines, and Yellow fever. There have been a number of vaccine trials in The Gambia some of, which have led to the inclusion of those vaccines in the routine EPI. Hepatitis B vaccine trial was conducted from 1986 to 1990, and the vaccine was included to the routine EPI in 1990. Hemophilus Influenzae type b trial was in 1993 to 1995 with its inclusion to the routine in 1997.
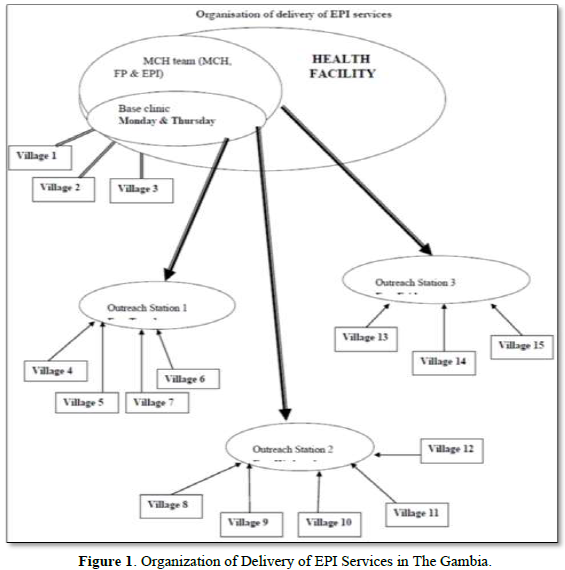
The Central EPI Unit, which is responsible for the overall management of the programme, is inadequately staffed and equipped. A recent review of the cold chain indicates current equipment is in urgent need of upgrading. More than half the equipment is more than ten years old. Storage capacity also needs to be expanded. Despite these constraints, the EPI has been very successful and percentage coverage is high. There are 196 outreach stations (key villages). Each outreach station serves 6-9 satellite villages as seen in Figure 1.
In the Gambia, the Multiple Indicator Cluster Surveys (MICS) conducted in 2000, 2010, and 2018 showed immunization coverage per antigen in the Kanifing Municipality. In 2000, the coverage for BCG was 93.3%; Penta3 63.8%; OPV3 80.0%; Measles 88.6%, and fully immunized before aged 12 months 57.1% [19]. In 2010, the coverage for BCG was 98.2%; Penta3 92.6%; OPV3 92.8%; Yellow fever 92.1%; Measles 92.5%; and fully immunized before aged 12 months 85.3% [20]. In the year 2018, coverage for BCG was 96.9%; Penta3 90.4%; OPV3 88.2%; Pneumo3 89.9%; Rota2 89.4%; IPV2 33.5%; Yellow fever 80.9%; Measles -Rubella1 83.5%; Measles-Rubella 2 89.3%; and fully immunized before aged 12 months 92.8% [21].
Unlike the MICS, The Gambia Conducted, two (2) Demographic Health Surveys (DHS) in 2013 and 2019-20. The coverage for BCG was 95.1%; Penta3 82.7%; OPV3 83.4%; Measles 84.3%; and fully immunized before 1 year of age 70.9% [22], while in 2019-20, the coverage for BCG was 98.0%; Penta3 86.0%,; OPV3 85.9%; IPV1 85.1%; PCV3 86.5%; Rota2 90.1%; Yellow Fever 85.8%; Measles-Rubella1 84.9%; fully immunized before aged 12 months 76.9% [23].
The WHO Recommended Routine Immunizations for Children recommends all children to be vaccinated against tuberculosis, diphtheria, tetanus, pertussis, polio, measles, hepatitis B, Hemophilus influenzae type b, pneumococcal bacteria/disease, rotavirus, and rubella by the age of 12 months [14].
Despite all the efforts the governmental and non‑governmental institutes put in for 100% immunization coverage, there are still pockets of low coverage areas. The Gambia Expanded Immunization currently averts an estimated 2 to 3 million deaths every year. However, the proportion of the world’s children who receive recommended vaccines has remained steady for the past few years [13].
In accordance with World Health Organization (WHO) recommendations, children are deemed fully immunized if they have received the measles vaccine by the age of 12 months, three doses of the diphtheria, pertussis, and tetanus toxoids (DPT) vaccine, and three doses of the polio vaccine. The pentavalent vaccination (DPT plus Hep B and Hib) has taken the place of the old DPT vaccine when The Gambia started include Hemophilus influenza type B (HiB) and hepatitis B (HepB) as of 2007 [14].
According to World Health Organization data, by 2011, there were 83%, 84%, and 84% of people worldwide who had had three doses of DTP, one dose of measles vaccination, and three doses of polio vaccine, respectively. However, more than one-fifth of children worldwide, particularly those in low-income nations, were still at risk for vaccine-preventable morbidity and death at the age of 12 months because they had not received all of their recommended vaccinations [13].
In The Gambia, the immunization policy calls for BCG vaccine given at birth or at first contact, three doses of pentavalent (DPT-HepB-Hib) vaccine and the newly added pneumococcal conjugate vaccine (PCV) vaccine given at approximately 4, 8, and 12 weeks of age, four doses of oral polio vaccine given approximately at 0-2, 4, 8, and 12 weeks of age, and measles vaccine given at or soon after reaching 9 months of age [23]. Within a year of a child's age, it is advised that they receive all of these vaccinations.
The relevance of the study depicts various population-based surveys that have indicated low coverage within the Kanifing Municipality and thus the study avails the researcher the opportunity to delve into why such coverages are low when it is predicted that with adequate knowledge of the implication of the immunization program the acceptance would be higher. However, sporadic cases of measles have been registered in the Gambia.
MATERIALS AND METHODS
A cross-sectional community-based study was adapted using the WHO (30X7) EPI cluster sampling survey methodology, as described in the 1991 WHO manual titled “Immunization Coverage Cluster Survey-Reference Manual” [24,25]. The Survey was conducted in the Kanifing Municipality region of The Gambia with a sample of 30 clusters of 10 households each to give the municipality- specific coverage estimates. A total of 300 households was enlisted in this study of which 298 children were assessed for determining their immunization status. The study recruited all children born from 7th March 2021 to 7th March 2022 for children 12 -23 months and for children 0-11 months respectively and the study was conducted from the 7th March to 7th April 2023.
Description of the Study Area
Kanifing Municipality is one of the eight Local Government Areas (LGAs) of The Gambia. It has a population of 322,735 (2003 Census) representing about 24 percent of the country's total population. With a land surface of 75.5 square kilometers and population density of 4,478 persons per square kilometer, the municipality is considered to be the most densely populated in The Gambia. Between 1993 and 2003, the population increased by 15 percent (Figure 2).

Selection of Cluster for the Study
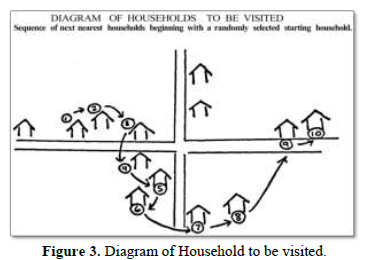
A list of all settlements was obtained with their respected population. The population was arranged in a cumulative frequency. A cluster interval was obtained by dividing the total population by 30. To obtain the first random number, a random number less than the cluster interval was generated by using the random number generator using https://www.calculator.net/random-number-generator.html which was 5,523. The first cluster in an area under population census data for Kanifing Municipality having a cumulative frequency equal to or more than 5,523 was picked up from the cluster and subsequent clusters selected by adding the cluster interval (5,523), that is, (5523 +12,571=18,094). The second cluster was the settlement having a cumulative frequency equal to or more than 18,094. Thus, in this manner, 30 clusters were selected. The first household was selected randomly and every next household was studied in sequence, until a total of ten eligible children in the age group of 12-23 months were covered as shown in the adapted diagram from WHO manual titled “Immunization Coverage Cluster Survey-Reference Manual” [24] (Figure 3).
Inclusion and Exclusion Criteria
All parents with eligible children born from 7th March 2021 to 7th March 2022 12-23 months old children and 0-11 months old children respectively. Parents that were excluded were those that were sick (ill health) or have cognitive inability (mental illness/memory loss or trouble remembering) to respond to questions.
Data Collection
The study collected data from parents of children aged 12-23 months in selected households using Coverage survey tool adapted from the 1991 WHO manual.
Data Analysis
The study analyzed data on childhood immunization coverage in Kanifing Municipality using Microsoft Excel a simple proportion were calculated of those children who received a particular vaccine against the number of children surveyed using the coverage survey tool adapted from the 1991 WHO manual and no tests of significance performed.
RESULTS
Infant Welfare Card (IWC) was available to 287 (95.7%) children surveyed aged 12-23 months old. Of the total children (N=287) 74.6% were fully immunized before 12 months while 80.5% were fully immunized by 24 months. Children who were partially immunized account for 56 (19.5%).
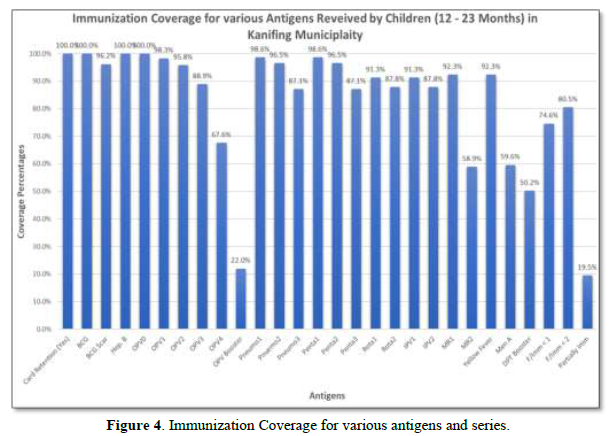
Overall, 100% (287/287) of the children received BCG; 88.9% (255/287) had received OPV3; 87.1% (250/287) had received PCV 3; 87.1% (250/287) had received Penta3; 87.8% (252/287) received IPV2; 87.8% (252/287) had received Rota2; 92.3% (265/287) had received Measles-Rubella first dose and 92.3% (265/287) had received Yellow fever (Table 4).
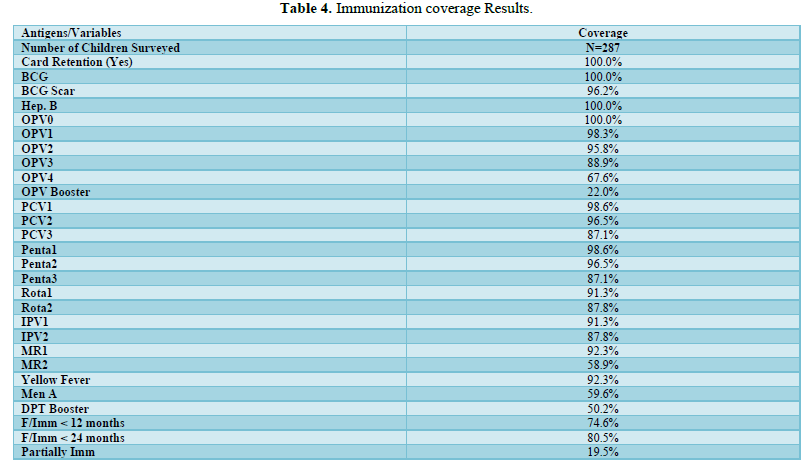
Coverage rates decline for subsequent doses of OPV, PCV, Penta, IPV, Rota, and Measles-Rubella. OPV0 to OPV4 coverage rates declined from 100% OPV0 to 88.9% OPV3; PCV1 from 98.6% to 87.1% PCV3; Penta1 from 98.6% to 87.1% Penta3; Rota1 from 91.3% to 87.8% Rota2; IPV1 from 91.3% to 87.8% IPV2; and MR1 from 92.3% to MR2 58.9%. Measles-Rubella has the highest decline as depicted above (Table 5).
The proportion of children who started certain vaccines but did not complete the next intended vaccines was 7.7% for BCG to MR1; 11.7% for Penta1 to Penta3; 9.6% for OPV1 to OPV3 and 6.4% for Penta1 to MR1 as shown in Tables 6-9 below (Figure 4).




Reasons for Children Partially Immunized
The respondents/Parents who had not completed their children’s vaccination were further asked for the reason that had caused it. The reasons were classified into three (3) broad perspectives namely (i) lack of information (ii) lack of motivation and (iii) obstacles (Table 10).
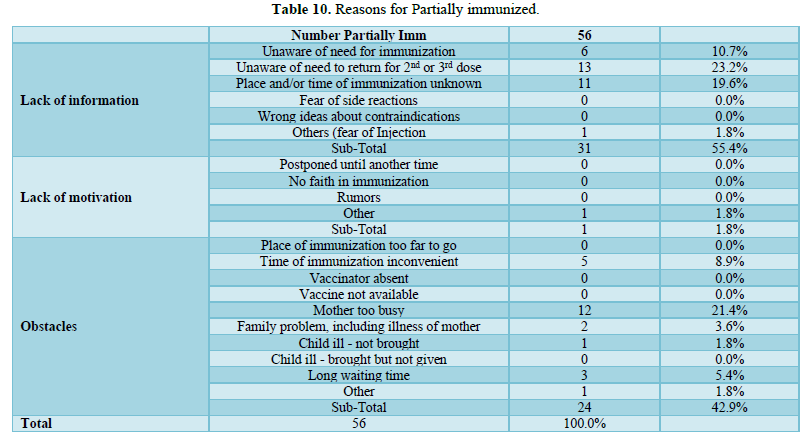
Out of the 56 (19.5%) children partially immunized/vaccinated, 13 (23.2%) were unaware of the need to return for a second or third dose; 11 (19.6%) said that the place and/or time of immunization was unknown; 12 (21.4%) said mothers were too busy while 6 (10.7% said they were unaware of the need for immunization (Figure 5).
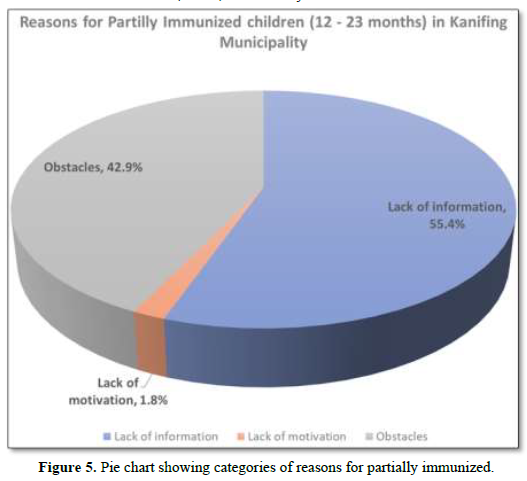
Thirty-one (55.4%) describe lack of information for not completing their children’s vaccination; 1 (1.8%); lack of motivation and 24 (42.9%) had various obstacles that warranted their children to complete their immunization status.
DISCUSSION
The majority of morbidity and death in children are caused by infectious illnesses. Immunization is one of the simple, low-cost techniques for ensuring a child's health and wellbeing. It is a great objective to immunize kids against diseases like measles, polio, diphtheria, pertussis, tetanus, hepatitis B, and tuberculosis that cause morbidity and death in children [2].
According to World Health Organization data, by 2011, there were 83%, 84%, and 84% of people worldwide who had had three doses of DTP, one dose of measles vaccination, and three doses of polio vaccine, respectively. However, more than one-fifth of children worldwide, particularly those in low-income nations, were still at risk for vaccine-preventable morbidity and death at the age of 12 months because they had not received all of their recommended vaccinations [13].
Despite all the efforts the governmental and non‑governmental institutes put in for 100% immunization coverage, there are still pockets of low coverage areas. The Gambia Expanded Programme on Immunization services are offered free in public health facilities private clinics and Hospitals, but despite rapid increases, the immunization rate remains low in some areas.
The study did not delve into the reasons if COVID-19 had any influence with the results of the current study and it was not a point of reference as it pertains to the study, however, it would have been crucial to determine if the emergence of COVID 19 has impact on the routine immunization coverage, thus there should be a need to conduct further research on. It is a known fact that COVID 19 has indeed decreased the attendance of mothers to clinics which ultimately affect immunization coverage. This study did not review the impact of COVID19 in relation to the impact of immunization coverage in Kanifing Municipality and vaccine hesitancy has not been a reference point in this study.
It is however to note that despite the study did not assess the impact of COVID-19 on the immunization program, it is important to emphasized that, directly and indirectly, the COVID-19 pandemic has had a catastrophic effect on many facets of life throughout the world. Managing the massive number of severely sick patients and deaths puts a strain on healthcare facilities and personnel. As of right now, a number of studies have documented a drop-in vaccination rates during the epidemic. According to WHO reports, delays in primary vaccination programs have been observed in at least 68 countries worldwide, affecting over 80 million children [26]. There has been a notable decrease in the ordering and administration of vaccines in various US states [27,28].
During the COVID-19 pandemic lockdown [29], the average daily vaccination visits in Karachi, Pakistan, fell by 52.8% as compared to the baseline. Immunization programs and child healthcare services were significantly impacted in sub-Saharan Africa [30] Several studies in Saudi Arabia during the epidemic revealed a reduction of almost 25% [31,32].
In comparison to data recorded prior to the COVID-19 interruption, there was an overall, modest decline of 13.4% in the average monthly attendance of children at immunization clinics during a 3-month period of the pandemic, according to a study done in The Gambia on the impact of the pandemic on the uptake of immunization services in rural Gambia. In comparison to the pre-COVID-19 baseline period, there was a 38.3% decrease in the average monthly vaccination antigen delivery during the COVID-19 interruption period. The decline in the mean monthly vaccination rate throughout the COVID-19 shutdown was most noticeable for vaccinations administered early in life, including BCG, birth dose Hep B, Penta1, OPV1, and PCV1 [33].
Potentially fatal childhood infections will resurface if children's primary immunization schedules are disrupted. This would undermine the current efforts to stop these VPDs. According to a benefit-risk analysis research conducted in Africa, the additional risk of COVID-19-related deaths at vaccination clinics is greatly outweighed by the deaths avoided by supporting routine children's vaccines. For every COVID-19 fatality linked to an illness contracted during a normal clinic visit, 84 fatalities in children may have been avoided by receiving standard childhood vaccinations [34].
As eluded earlier in the introduction all the population-based surveys have indicated the lowest coverage in Kanifing Municipality and there was the need to review why and thus the study also had a KAPP component to determine the factors for low coverage. The findings of this study revealed that 287 (95.7%) children surveyed aged 12-23 months old had Infant Welfare Card (IWC) and out of which from the total children (N=287) 74.6% were fully immunized before 12 months while 80.5% were fully immunized by 24 months. Children who were partially immunized account for 56 (19.5%).
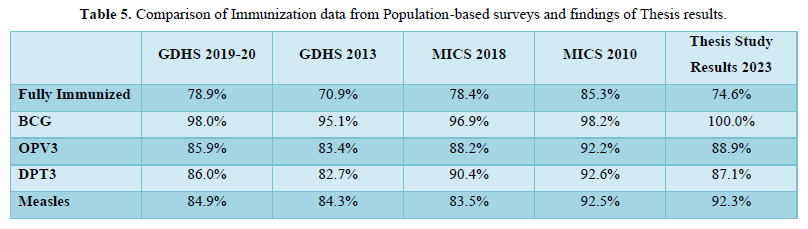
In The Gambia, the Multiple Indicator Cluster Surveys (MICS) conducted in 2000, 2010, and 2018 showed fully immunization coverage before the before 12 months old in the Kanifing Municipality varying from 57.1% [19], 85.3% [20] and 92.8% [21] respectively and the two (2) Demographic Health Surveys (DHS) in 2013 and 2019-20 showed 70.9% [22], while in 2019-20, indicated 76.9% [23]. Both results from the GDHS (2013 and 2019-20) were not far from the findings of the study.
Similar studies conducted by Martin Nyaaba Adokiya [16], 2016, revealed that out of 600 children survey, 89,5% were fully immunized and another study by Elias legesse and Worku Dechasi [17] in 2013 assessing child immunization coverage and its determination in Sinana district, Southeast Ethiopia revealed that 76.8% of Children aged 12 to 23 months were fully vaccinated by card plus history. Another cross-sectional survey was conducted in Dechang , West Region Cameroun during a polio outbreak on vaccine coverage and determinants in incomplete vaccination in children aged 12-23 months revealed that 85.9% of the children were fully immunized [18].
The study findings regarding the overall who received BCG was 100%; OPV3 88.9%; PCV3 87.1%; Penta3 87.8%; IPV2 87.8%; Rota2 92.3%; Measles-Rubella1 92.3% and Yellow Fever 92.3%. The results found out from this study was not much of a difference from the results of previous surveys conducted in The Gambia. In 2000, the coverage for BCG was 93.3%; Penta3 63.8%; OPV3 80.0%; Measles 88.6%, [19]. In 2010, the coverage for BCG was 98.2%; Penta3 92.6%; OPV3 92.8%; Yellow fever 92.1%; Measles 92.5% [20].
In the year 2018, coverage for BCG was 96.9%; Penta3 90.4%; OPV3 88.2%; Pneumo3 89.9%; Rota2 89.4%; IPV2 33.5%; Yellow fever 80.9%; Measles -Rubella1 83.5%; Measles-Rubella 2 89.3% [21]. Unlike the MICS, coverage for BCG was 95.1%; Penta3 82.7%; OPV3 83.4%; Measles 84.3% [22], in 2019-20, the coverage for BCG was 98.0%; Penta3 86.0%,; OPV3 85.9%; IPV1 85.1%; PCV3 86.5%; Rota2 90.1%; Yellow Fever 85.8%; Measles-Rubella1 84.9% [23]. This was further collaborated with the study conducted in Dechang, West Region Cameroun in that 98.8% had Measles; 92.8% Penta3; 91.6% OPV3; 90% Measles; 90% yellow fever [18].
The findings of this study further revealed that Coverage rates decline for subsequent doses of OPV, PCV, Penta, IPV, Rota, and Measles-Rubella. OPV0 to OPV4 coverage rates declined from 100% OPV0 to 88.9% OPV3; PCV1 from 98.6% to 87.1% PCV3; Penta1 from 98.6% to 87.1% Penta3; Rota1 from 91.3% to 87.8% Rota2; IPV1 from 91.3% to 87.8% IPV2; and MR1 from 92.3% to MR2 58.9%. Measles-Rubella has the highest decline as depicted above. The proportion of children who started certain vaccines but did not complete the next intended vaccines was 7.7% for BCG to MR1; 11.7% for Penta1 to Penta3; 9.6% for OPV1 to OPV3 and 6.4% for Penta1 to MR1.
The respondents/Parents who had not completed their children’s vaccination were further asked for the reason that had caused it. The reasons were classified into three (3) broad perspectives namely (i) lack of information (ii) lack of motivation and (iii) obstacles. Out of the 56 (19.5%) children partially immunized/vaccinated, 13 (23.2%) were unaware of the need to return for a second or third dose; 11 (19.6%) said that the place and/or time of immunization was unknown; 12 (21.4%) said mothers were too busy while 6 (10.7% said they were unaware of the need for immunization. Thirty-one (55.4%) describe lack of information for not completing their children’s vaccination; 1 (1.8%); lack of motivation and 24 (42.9%) had various obstacles that warranted their children to complete their immunization status.
The findings of this study also collaborated with the survey findings of a survey conducted in rural Gambia regarding COVID-19, of which 40% of respondents stated that transportation was a problem. This could be because interstate travel was restricted by lock downs and curfews implemented during the epidemic. It could also be the result of delays in the ordering and distribution of vaccines, particularly in regions where widespread immunization programs are underway. In the future, initiatives like providing passes or expanding home care services should be prioritized in order to lower this barrier to necessary preventative therapies [33].
In addition, a lot of parents refrained from bringing their kids, especially infants, to EPI clinics out of concern that they would get COVID-19 during the vaccination clinics [35].
These findings are also similar with the findings from the study conducted in Dechang, West Region Cameroun wherein 14.1% were partially immunized. Out of those partially immunized the reason were mothers too busy accounted for 32.2% (n=22) [18] and the study from conducted by Martin Nyaaba Adokiya et al, 2016, revealed that out of 600 children survey, 89,5% were fully immunized and another study by Elias legesse and Worku Dechasi in 2013 assessing child immunization coverage and its determination in Sinana district, Southeast Ethiopia revealed 9.5% were partially immunized while 1.0% had not received any vaccine [16]. In the same study, it has revealed that of the 63 children not fully immunized, 57.1% reported time was not convenient and 14.3% said the place of immunization was not known or the mother was too busy.
CONCLUSION
Infectious illnesses are the primary cause of morbidity and death in children, with immunization being a crucial technique for ensuring their health and well-being. In the Gambia, the Expanded Programme on Immunization services are offered free in public health facilities, private clinics, and hospitals, but the immunization rate remains low in some areas. The study revealed that 287 (95.7%) children aged 12-23 months old had Infant Welfare Card (IWC), with 74.6% being fully immunized before 12 months and 80.5% being fully immunized by 24 months.
Children who were partially immunized account for 56 (19.5%). The study also found that coverage rates declined for subsequent doses of OPV, PCV, Penta, IPV, Rota, and Measles-Rubella. Out of the 56 (19.5%) partially immunized children, 23.2% were unaware of the need to return for a second or third dose, 19.6% said the place and/or time of immunization was unknown, 22.4% said mothers were too busy, and 10.7% said they were unaware of the need for immunization. Thirty-one (55.4%) described a lack of information for not completing their children's vaccination, 1.8% had a lack of motivation, and 24 (42.9%) had various obstacles that warranted their children to complete their immunization status. In conclusion, the immunization rate in the Gambia remains low, with a need for increased vaccination coverage and better immunization practices.
IMPLICATIONS
The healthcare professionals should be able to effectively explain to parents the value of vaccinations, their safety, and the repercussions of not adhering to the recommended schedules. Parents and healthcare professionals alike need to be aware of the issue with declining immunization rates. The findings of this study demonstrated how crucial healthcare professionals are in influencing parents' views and immunization habits.
- World Health Organization (2018) Million children miss out on lifesaving measles, diphtheria and tetanus vaccines in 2018.
- Chaudhary V, Kumar R, Agarwal VK, Joshi HS, Sharma M (2010) Evaluation of Primary immunization coverage in an urban area of Bareilly city using Cluster Sampling Technique. Natl J Integr Res Med 1(4): 10-15.
- Harris JB, Gacic-Dobo M, Eggers R, Brown DW, Sodha SV (2014) Global routine vaccination coverage, 2013. MMWR Morb Mortal Wkly Rep 63(46): 1055.
- World Health Organization (2005) GIVS: Global immunization vision and strategy: 2006-2015.
- Vohra (2023) Immunization coverage and its determinants among 12-23 months old children of Lucknow.
- Bhonsla SK, Bhardwaj A, Mittal A, Singla G, Garg S, et al. (2019) Determinants of immunization coverage among 12-23 months children: A study from Haryana. Indian J Community Health 31(1): 78-83.
- AbouZahr C, Boerma T (2010) Five years to go and counting: Progress towards the Millennium Development Goals. Bull World Health Organ 88(5): 324.
- WHO (2009) State of the world’s vaccines and immunization. World Health Organization Geneva.
- UNICEF (2019) UNICEF launches Vaccines work campaign to inspire support for vaccines. Zuletzt abgerufen am 21:2020.
- Touray E, Barrow A, Kinteh B, Badjie M, Nget M, et al. (2021) Childhood vaccination uptake and associated factors among children 12-23 months in rural settings of the Gambia: A community-based cross-sectional study. BMC Public Health 21(1): 1740.
- Sowe A, Johansson K (2019) Disentangling the rural-urban immunization coverage disparity in The Gambia: A Fairlie decomposition. Vaccine 37(23): 3088-3096.
- Gooding E, Spiliotopoulou E, Yadav P (2019) Impact of vaccine stockouts on immunization coverage in Nigeria. Vaccine 37(35): 5104-5110.
- Immunization coverage (2023).
- World Health Organization (2023) WHO recommendations for routine immunization.
- Mohamud AN, Feleke A, Worku W, Kifle M, Sharma HR (2014) Immunization coverage of 12-23 months old children and associated factors in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health 14(1): 865.
- Adokiya MN, Baguune B, Ndago JA (2017) Evaluation of immunization coverage and its associated factors among children 12-23 months of age in Techiman Municipality, Ghana, 2016. Arch Public Health 75(1): 28.
- Legesse E, Dechasa W (2015) An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatrics 15(1): 31.
- Russo G, Miglietta A, Pezzotti P, Biguioh RM, Mayaka GB, et al. (2015) Vaccine coverage and determinants of incomplete vaccination in children aged 12–23 months in Dschang, West Region, Cameroon: A cross-sectional survey during a polio outbreak. BMC Public Health 15(1): 630.
- The World Bank (2023) Gambia - Multiple Indicator Cluster Survey 2000.
- International Household Survey Network (2023) Gambia, The - Multiple Indicator Cluster Survey 2010.
- UNICEF Gambia (2019) The Gambia Multiple Indicator Cluster Survey 2018.
- GBos TGB of S, International ICF (2014) The Gambia Demographic and Health Survey 2013.
- GBoS GB of S, ICF (2021) The Gambia Demographic and Health Survey 2019-20.
- World Health Organization (2020) Training for mid-level managers (MLM): Module 7: The EPI coverage survey.
- Murthy BN, Radhakrishna S, Venkatasubramanian S, Periannan V, Lakshmi A, et al. (1999) Lot quality assurance sampling for monitoring immunization coverage in Madras City. Indian Pediatr 36: 555-558.
- Alhusayn K, Alsulaiman T, Abdulkarim A, Sultana H, Jnaid H, et al. (2023) COVID-19 pandemic impact on primary immunization uptake. J Family Med Prim Care 12(6): 1172-1178.
- Santoli JM (2020) Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration-United States, 2020. MMWR Morb Mortal Wkly Rep 69(19): 591-593.
- Murthy BP, Zell E, Kirtland K, Jones-Jack N, Harris L, et al. (2021) Impact of the COVID-19 pandemic on administration of selected routine childhood and adolescent vaccinations-10 US jurisdictions, March-September 2020. MMWR Morb Mortal Wkly Rep 70(23): 840.
- Chandir S, Siddiqi DA, Setayesh H, Khan AJ (2020) Impact of COVID-19 lockdown on routine immunization in Karachi, Pakistan. Lancet Glob Health 8(9): e1118-e1120.
- Buonsenso D, Cinicola B, Kallon MN, Iodice F (2020) Child healthcare and immunizations in sub-Saharan Africa during the COVID-19 pandemic. Front Pediatr 8: 517.
- Alrabiaah AA, Alshaer AH, Estrella SMC, Inclan KAS, Aljammaz HA, et al. (2020) Effects of the Coronavirus disease 2019 pandemic on routine pediatric immunization coverage rates at the main University Hospital in Saudi Arabia. Saudi Med J 41(11): 1197.
- Alsuhaibani M, Alaqeel A (2020) Impact of the COVID-19 pandemic on routine childhood immunization in Saudi Arabia. Vaccines 8(4): 581.
- Osei I, Sarwar G, Hossain I, Sonko K, Ceesay L, et al. (2022) Attendance and vaccination at immunization clinics in rural Gambia before and during the COVID-19 pandemic. Vaccine 40(44): 6367-6373.
- Abbas K, Procter SR, Van Zandvoort K, Clark A, Funk S, et al. (2020) Routine childhood immunization during the COVID-19 pandemic in Africa: A benefit-risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob Health 8(10): e1264-e1272.
- The Chronicle Gambia (2020) In Gambia, Mothers Keep Children from Immunization Due to COVID-19 Vaccine Fear.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6
-
Table 7
-
Table 8
-
Table 9
-
Table 10















QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)


