119
Views & Citations10
Likes & Shares
Introduction: Methicillin resistant Staphylococcus aurous (MRSA) is a threat to both the hospital and community. Community-acquired methicillin resistant Staphylococcus aureus (CAMRSA) is increasing rapidly leading to increase in morbidities and mortalities rate in the world.
RESEARCH PROBLEM
The fact that there are always various events for people to show-off, from weddings, graduation parties, reunions, anniversaries, business meetings, dinner party and so on. These events are usually conducted in halls that provide convenient facilities for guests than would have been achieved in a home or office. In addition, an average football fan in Nigeria may not even be able to afford a satellite TV to watch matches of their favourite clubs, while even if they can afford, they prefer viewing centers. This is because it gives them the opportunity to team up with other club fans. Crowded environments have been reported to significantly increase the risk of MRSA colonization [7]. According to Al-Ruaily [8] Colonization has been reported as an important step in the chain of events that lead to S. aureus infections. CAMRSA is emerging as a serious threat to public health worldwide and has significantly increased morbidity and mortality rate of patients along with the increased length of hospital stay.
AIM AND OBJECTIVES
Aim of the Study
The aim of study was to survey for the presence community-acquired methicillin resistant Staphylococcus aureus from Event and Viewing Centers in Kano Metropolis, Nigeria.
Objectives of the Study
- To isolate and identify Methicillin resistant Staphylococcus aureus from human hands, noses, fomites, objects and indoor air of some Event and Viewing Centers.
- To determine the susceptibilities of the isolates to various antibiotics.
- To determine the distribution of Staphylococcus aureus and MRSA from both Event and Viewing Centers.
METHODOLOGY
Study Area
This study was carried out at some event and viewing centers of Kano Metropolis, Kano State, Nigeria. It’s located between latitudes 11°52'N and 12°07'N and longitudes 8°24'E and 8°38'E. It’s a conurbation of eight Local Government Areas (LGAs) around main city, which metamorphose to form the present Kano metropolis. The LGAs are Dala, Fagge, Gwale, Kano Municipal, Kumbotso, Nasarawa, Tarauni and Ungoggo. These eight LGAs formed the study area for this study.
Study Design
A cross Sectional study
Ethical approval
Ethical approval for the study was obtained from the ethics committee of Kano State Censorship Board, in 15 November, 2019; an ethical approval to conduct the study was issued.
SAMPLES COLLECTION
Swab stick Sampling
A total of 588 Samples were collected from apparently healthy humans’ hand and nasal mucosa, using sterile swab sticks [9]. Samples were also collected from the surfaces of door handles, Handset keypads, locker/drawer handles, surfaces like Tables, Air conditioners, TV Screen and TV set remote control. Surfaces was swabbed using a sterile swab sticks, and the sampled swab sticks were put in to polyethylene bags inside ice box. All the samples were immediately taken to Microbiology Laboratory, Department of Microbiology, Bayero University Kano, for microbiological analysis as described by CLSI, (2018).
Indoor Air Sampling
Sampling were conducted twice a day early before starting the Event and Viewing and during the Event and Viewing, in accordance with the direction of prevailing winds, on the height of 1.5m above the ground level to maintain uniform collection of air samples. A total of 192 samples were collected in all Event and Viewing Centers. To collect the samples, Mannitol Salt Agar (MSA) plates were exposed for 30 min at the height of 1.5m above the ground level. After the exposure, the plates were taken to the Microbiology Laboratory, Department of Microbiology, Bayero University Kano, and incubated at 37°C for 24 h [10].
Bacterial Isolation
All Swab stick samples were also streaked on a prepared Mannitol Salt Agar (MSA) plate in a Zig zag motion and incubated at 37°C for 24 h. After overnight incubation on Mannitol Salt Agar, yellow colonies were picked and sub cultured into sterile Blood Agar (BA) plate and further incubated at 37ºC for 24 h, the organisms formed milky and some yellowish colonies and changing the red bloody color of the medium to yellow with hemolysis on MSA and BA respectively are characterizing as S. aureus and used for further analysis (Hilliard and Reddy, 2018) (Table 1).

Antibiotics Susceptibility Testing
Antibiotics susceptibility testing was carried out using the disc diffusion method (CLSI, 2018). The culture inoculum was first standardized by emulsifying a loopful of discrete colonies of S. aureus in 3 ml of physiological saline and form a standard culture suspension. The culture suspension was adjusted and a turbidity equivalent to 0.5 Mcfarland Standard (equivalent to 1.5 x 108 cfu/ml). Mueller Hinton agar (MHA) plates were then inoculated with the test bacteria (0.5 Mcfarland turbidity standard) using a sterile swab stick. The plates were allowed to dry for 10 min and then commercial antibiotics discs, gentamicin (30µg), cefoxitin (30µg), ceftriaxone (30µg), cefuroxime (30µg), ceftazidime (30µg), ofloxacin (5µg), amoxicillin (20µg), chloramphenicol (30µg) and erythromycin (5µg) were applied aseptically to the surface of the agar. After 30 min of applying the discs, the plates were inverted, and incubated at 37°C for 24 h. The zone of inhibition was measurement and interpreted as resistant and sensitive based on the guidelines of CLSI, (2018).
Detection of Community Acquired Methicillin Resistant Staphylococcus aureus (CAMRSA)
A 0.5 Mc Farland standard suspension of the isolate was made and a lawn culture was done on MHA plate. Cefoxitin 30μg discs were placed and plates were incubated at 37°C for 24 h and zone diameter was measured. An inhibition zone diameter ≤21 mm was reported as methicillin resistant and ≥22 mm was considered as methicillin susceptible (CLSI, 2018).
Statistical analysis
Chi-square was used to see if there was a significant difference in the occurrence of S. aureus and MRSA isolated from event and viewing centers. Calculated p-value of >0.05 were considered to be statistically not significant.
RESULT AND DISCUSSION
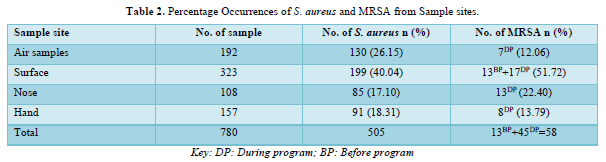
Refer to the Table 2 showing the overall occurrences of S. aures and MRSA. Of total 780 bacterial samples survey from different event and viewing center within Kano metropolitan, Surface has highest number of 199(40.04) of Staphylococcus aureus with 30(51.72) Methicillin resistant strains in which viewing center showed the highest number of MRSA. Furthermore, the highest number of resistant strains in viewing and event center were all obtained during program, this was not surprising because aerosols contribute as a route of indirect transmission or surface contamination in congested places and consequently to a higher probability of cross infection [11] Of 58 Methicillin resistant Staphylococcus aureus (MRSA) isolates, 45(77%) were all detected during program, this was much higher than 13.2% recorded by [12] in a study conducted in Federal University Dutse, Jigawa State, Nigeria. Factors such as overcrowding and poor personal and environmental hygiene can all influence the viability of MRSA in an indoor environment [13].
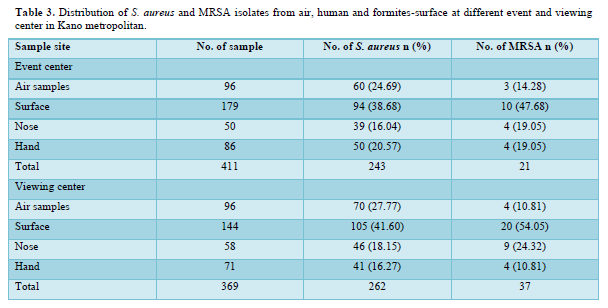
In Table 3 when comparing the number and percentages of S. aureus in the Event and Viewing Centers, the rate of S. aureus was higher in viewing centers 262(51.8%) compared with event centers 243(48.1%). However, no significant difference (P value = 0.764617). Likewise, if we look at the distribution of MRSA isolates between different event and viewing centers, we found them to be 37(63.8%) in viewing centers and 21(36.2%) in event centers out of a total 58. However, there is significant difference (P value = 0.032077) in the distribution of MRSA. This higher occurrence of S. aureus and MRSA in viewing centers could be due to various associated risk factors such as overcrowding, poor hygienic condition, antibiotic treatment, underlying immune-compromised conditions which predispose an individual to MRSA acquisition. These studies observed a decrease of contamination level in Event Centers than Viewing Centers this may be attribute to the proper structural design, good hygienic condition, restriction of movement and the people entering event centers are need, it may be responsible for the lower rate of S. aureus and MRSA in event centers. Since, the P value = 0.032077 is lower than 0.05, hence there is statistically difference between the MRSA isolated in Event and Viewing Centers. In this present study, most of the samples collected were from fomite-surfaces and has to be with highest isolates for both event and viewing centers in Kano metropolitan, the results are similar to those reported by [8]. Here, the result also shows that fomite-surfaces (door handle) are more prone to S. aureus. This might be due to high chances of contact with door handles and also S. aureus is a normal flora of the human skin and due to the fact that human being always interact with their environment, is possible that the organism can leave human body to live on his environment. It is was reported that microbes can persist on an-animate object for a long period of time ranging from less than a minute to about a month or more as reported by Kramer [13] in their work, they reported that some organism can persist for a long period on surfaces and air. Crowded environments have been reported to significantly increase the risk of MRSA colonization. Colonization has been reported as an important step in the chain of events that lead to S. aureus infections [7,8]. Methicillin resistance Staphylococcus aureus isolation rate from nasal, hand and fomite found in this study is similar to findings of Ghidey [14] which have suggested that nasal colonization is not the only route for pathogenesis of CA-MRSA infection and that skin-skin and skin-fomite contact could represent important transmission routes. Nasal carriage of MRSA is an important risk factor for subsequent MRSA infection and transmission as the bacterium is transmitted to the nares by contaminated hands and from surfaces where it can survive for months [15].
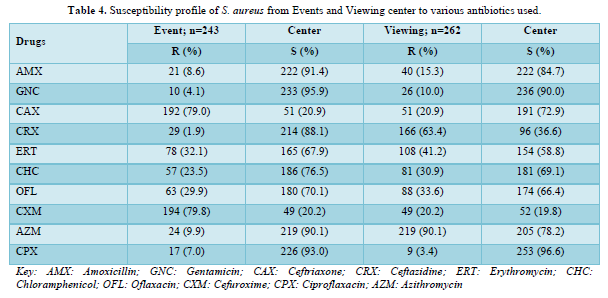
For the susceptibility test of S. aureus showed that ciprofloxacin and gentamicin had the greatest activity with 253/262 (96.2%) and 233/243 (95.9%) in viewing and event center respectively. In other hand cefuroxime from β-lactams antibiotics was the highest resistant antibiotic with 194/243(80.2) and 210/262(79.8%) in viewing and event center respectively (Table 4). Ciprofloxacin and gentamicin seem to be the only antimicrobial agent that showed the highest level of susceptibility against S. aureus in the study which is consistent with previous report by Ibrahim [16] and However, it was higher than those reported by Kadora [17] and Kumurya and Ado [18] in their study in Kano. Hence, these antibiotics may be used as the drug of choice for treating MDR-MRSA infections. However, frequent monitoring of their sensitivity and routine testing should be carried out. Use of ciprofloxacin and gentamicin should be limited to preserve their values. The high rate of resistance to cefuroxime, ceftriaxone, ceftazidime and erythromycin shows that these antibacterial agents would be unreliable and also most of the isolates showed resistance towards commonly β-lactams antibiotics. This agrees with previous reports that most isolates of S. aureus are resistant to a large number of commonly prescribed antibiotics [19]. Self-medication and indiscriminate use of antibiotics have severally been reported as promoters of antibiotic resistance and frequent administration of systemic antibiotics modified nasal S. aureus from MSSA to MRSA. Moreover, the differences in sensitivity profile of the bacteria isolates among the sources may be attributed to practices of self-medication, drug abuse and indiscriminate use of antibiotics. Similarly, Onanuga and Temedie [20] also confirmed the occurrence of high multiple antibiotic index in their study.
CONCLUSION
The study recorded the overall 505 S. aureus with 58 methicillin resistant, about half and quarter of resistant strains was recovered during programmed, this study provides a vital information of the presence of Community acquired methicillin resistant Staphylococcus aureus (CAMRSA). In addition to that it was found that Ciprofloxacin and Gentamicin was active against almost mediated CAMRSA isolates. Hence, the use of those antibiotics may be used as drugs of choice for treating MDR-MRSA infections.
RECOMMENDATION
Education /awareness on strict adherence to aseptic procedure and regular screening of event and viewing centers for the presence of MRSA to control colonization and infection. Also, proper building design of event and viewing centers are needed to aid ventilation and reduce overcrowding.
- Harkins CP, Pichon B, Doumith M, Parkhill J, Westh H, et al. (2017) Methicillin-resistant Staphylococcus aureus emerged long before the introduction of methicillin into clinical practice. Genome Biol 18 (1): 130.
- Bien J, Sokolova O, Bozko P (2011) Characterization of virulence factors of Staphylococcus aureus: Novel function of known virulence factors that are implicated in activation of airway epithelial pro inflammatory response. J Pathog 2011: 601905.
- ECDC (2017) Surveillance of antimicrobial resistance in Europe 2017. European Centre for Disease Prevention and Control.
- Koukos G, Sakellari D, Arsenakis M, Tsalikis L, Slini T, et al. (2015) Prevalence of Staphylococcus aureus and methicillin resistant Staphylococcus aureus (MRSA) in the oral cavity. J Oral Biol 60(9): 1410-1415.
- Lakhundi S, Zhanga K (2018) Methicillin-resistant Staphylococcus aureus: Molecular characterization, evolution, and epidemiology. Clin Microbiol Rev 31(4): 20-118.
- Abe AS, Inuwa B, Abbas H, Sule AM, Mohammed HA, et al. (2012) Identification and Characterization of Bacteria Air Pathogens from Homes in Zaria Metropolis. Int J Sci Technol 2(7): 443-446.
- Ugwu MC, Anie CO, Ibezim EC, Esimone CO (2016) Antimicrobial evaluation of methicillin-resistant Staphylococcus aureus nasal carriage amongst healthy students in Agbor, Delta State, Nigeria. J Clin Microbiol 7(2): 1-4.
- Al-Ruaily A, Khalil OM (2015) Detection of (mecA) gene in methicillin resistant Staphylococcus aureus (MRSA) at Prince A / Rhman Sidery Hospital, Al-Jouf, Saudi Arabia. J Med Gene Eng 3(3): 41-45.
- Clinical and Laboratory Standards Institute (2018) Performance standards for antimicrobial susceptibility testing approved standard M100-S23. Clinical and Laboratory Standards Institute, Wayne, PA. pp: 12-94.
- Cheesbrough M (2010) District Laboratory Practice in Tropical Countries. Cambridge University Press; pp: 45-70.
- Clinical and Laboratory Standards Institute (2018). Performance standards for antimicrobial susceptibility testing approved standard M100-S23. Clinical and Laboratory Standards Institute, Wayne, PA; p.12-94.
- Kobza J, Pastuszka JS Bra, Goszewska E (2018) Do exposures to aerosols pose a risk to dental professionals? J Med 68: 454-458.
- Mohammed B, Haruna I (2019) Assessment of indoor air bacterial load from some hospitals Dutse, Jigawa state. J Pure Appl Sci 12(2): 57-66.
- Kramer A, Ingeborg S, Kampf G (2006) How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis 6: 130.
- Ghidey F, Igbinosa O, Igbinosa E (2014) Nasal colonization of methicillin resistant Staphylococcus aureus (MRSA) does not predict subsequent infection in the intensive care unit. Beni-Suef. Uni J Basic Appl Sci 3: 81-86.
- Alaklobi F, Aljobair F, Alrashod A, Alhababi R, Alshamrani M, et al. (2015) The prevalence of community-associated methicillin-resistant Staphylococcus aureus among outpatient children in a tertiary hospital: A prospective observational study in Riyadh, Saudi Arabia. Int J Pedietr Adolesc Med 2: 136-140.
- Ibrahim A, Aminu AI, Abdullahi S, Usman MI (2017) Detection of Methicillin Resistant Staphylococcus aureus (MRSA) from hospital instruments. Uni J Microbiol 2(3): 11-17.
- Kadora I (2010) Antibiotic sensitivity patterns of hospital-acquired and community-acquired methicillin resistant Staphylococcus aureus. Theses, Dissertations and Capstones. Marshall University; pp: 100.
- Kumurya A, Ado B (2015) Prevalence of methicillin-resistant Staphylococcus aureus in AKTH: systemic review and meta-analysis. Afr J Clin Microbiol 14(3): 146-154.
- Okwu M, Sinat B, Wakeel A (2012) Prevalence of nasal carriage of community-associated methicillin resistant Staphylococcus aureus (CA-MRSA) among healthy primary school children in Okada, Nigeria. J Sci Res 2(4): 61-67.
- Onanuga A, Temedie TC (2011) Nasal carriage of multi-drug resistant Staphylococcus aureus in healthy inhabitants of Amassoma in Niger Delta region of Nigeria. Afri Health Sci 11(2): 176-181.
- Forbes BA, Sahm DF (2007) Weissfeld, Bailey and Scoots’s Diagnostic microbiology. Mosby Inc, Maryland Heights, MO, USA, 12th
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Pathology and Toxicology Research


