423
Views & Citations10
Likes & Shares

Impaction of multiple permanent teeth is rare condition and is often associated with Syndromes (like cleidocranial dysplasia) [6-8], metabolic, and hormonal disorders. While multiple impactions with no syndromic or systemic etiology is rare condition and little literature regarding them is available. Though less frequent but multiple impactions pose serious difficulty during treatment and its outcome depends on age of start of treatment, root formation stage, location and distance of teeth from occlusal plane.
In present study we aim to discuss two cases with multiple impactions in non-syndromic patients.
CASE REPORT 1
A 13 years old male patient reported with chief complain of multiple missing front teeth in upper arch and compromised esthetics. Patient had normal build, gait and posture with no previous medical, dental or family history. Patient had convex facial profile and no facial asymmetry was seen. Radiographic examination of the skull, chest and clavicles were normal. Ophthalmological and neurological examination presented no pathological symptoms. Patient revealed no signs of syndromes, skeletal abnormalities, systemic disorders or mental retardation. On further enquiry it was found that the front deciduous teeth in upper arch had exfoliated 2 years back and permanent teeth had not erupted. While lower front deciduous teeth had fallen and permanent teeth had erupted normally.
On clinical examination it was found that 20 teeth were present out of which upper central and lateral incisors were missing, lower incisors and all first molars were permanent teeth and rest were deciduous teeth. Lower incisors seemed to be partially erupted. Overjet and overbite could not be assessed. Maxillary and mandibular arch form were oval and symmetrical (Figure 1 & Table 1).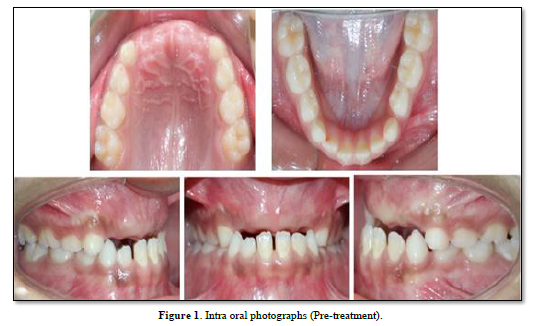

Patient was advised OPG for further radiographic evaluation. The panoramic radiograph of the patient revealed multiple impacted teeth in maxilla and mandible. Also, multiple retained deciduous teeth in maxilla and mandible. Enamel and pulp chambers appeared normal. Roots of central and lateral incisors were complete while that of canines and premolars were partially formed (Figure 2).

It was planned to assist the eruption of central and lateral incisors in maxilla by surgical exposure and orthodontic traction at intermittent monitoring periods.
After 1 year of treatment patient discontinued the treatment. Patient returned to our clinical setup after a year at age of 15 years. Clinically 4 upper incisors had erupted partially and were in crossbite with lower incisors. The deciduous canines and molars in maxilla and mandible were present and were not mobile. Permanent second molars were present in all the quadrants. The panoramic radiograph was done and it was found that roots of upper and lower premolars and canines were almost completely formed and there was almost no resorption of roots of deciduous teeth (Figures 3 & 4).

ASE REPORT 2
An 18 years old female patient reported with chief complain of crowding in upper and lower arch. Patient had an athletic build, normal gait and posture with no previous medical or dental history. She had no relevant family history and this was her first dental visit. Patient had convex facial profile with apparently symmetrical face. Slight soft tissue asymmetry was present on smiling. Patient revealed no signs of syndromes, skeletal abnormalities, systemic disorders or mental retardation. Intelligence was subjectively normal. Head hair and body hair were clinically normal.
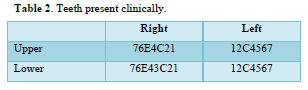
On clinical examination it was found that she had multiple retained deciduous teeth along with multiple impacted teeth in upper and lower arches of which patient was un aware of. Intraorally 29 teeth were present. Retained deciduous teeth present were canines in all quadrants and 2nd deciduous molars in upper and lower right quadrants.
Teeth impacted were upper right and left canines and right 2nd premolar. In lower arch teeth impacted were lower left canine and right 2nd premolar. Overjet of 1mm and overbite of 2mm were present. Maxillary and mandibular arch form were oval and symmetrical (Table 2 & Figure 5).

Patient was advised panoramic radiograph for further assessment. The panoramic radiograph of the patient revealed multiple impacted teeth in maxilla and mandible. Also, multiple retained deciduous teeth in maxilla and mandible. Enamel and pulp chambers appeared normal. Roots of all impacted teeth were completely formed. And some resorptions of deciduous teeth were present (Figure 6). The treatment plan selected in this case was surgical exposure and orthodontic traction for eruption of impacted teeth. If patient does not respond to orthodontic traction, then surgical extraction and prosthetic treatment would be required.
DISCUSSION
Impaction of multiple teeth is a rare condition and mostly present with some underlying systemic disease or associated syndromes. Etiology for impacted teeth varies from lack of space, early loss or prolonged retention of deciduous teeth to presence of some physical barrier [3,9,10]. Third molars and maxillary canines are most commonly impacted teeth, however in present cases there was impaction of maxillary central and lateral incisors along with canines and premolars in both the arches. Such condition is very rare and should be examined for associated systemic diseases or syndromes like cleidocranial dysplasia, Down syndrome, Gardener’s syndrome etc. [6,7,11,12].
Conditions that cause lacking of eruptive forces could be due to either general, endocrinal, neurogenic or mucosal and bone disorder. While Conditions associated with retained teeth are: hemifacial atrophy, hypopituitarism, hypothyroidism, gingival fibromatosis, cleft palate etc. [7,9]. In Cases mentioned in this article, no features of any disorder, systemic diseases or syndromes were found. Further medical history and examination of patients did not present any signs of metabolic and nutritional disorders. The above conditions were thus excluded.
In case 1 it seems that there was idiopathic cause for failure of eruption of teeth in upper and lower arches. Since the roots of maxillary incisors were complete, surgical exposure and orthodontic traction was selected as treatment plan, after which incisors erupted as the treatment progressed. As the patient’s age advanced it was found that the canines and premolars were also impacted and there was no root resorption of deciduous teeth. A Similar case report by Sujatha [13] with multiple impactions of permanent teeth described alike condition that was not associated with any syndrome.
In case 2 over retained deciduous teeth seem to be the cause of multiple impactions, if at right age deciduous teeth had been extracted spontaneous eruption of the permanent teeth might have taken place. Lack of space in dental arches caused rotation of tooth buds contributing to impaction.
Multiple complications related to impacted teeth include root resorption, associated pathologies, aberrant root morphology and location leading to poor prognosis for their eruption. In these cases, interdisciplinary approach of treatment including orthodontist, oral surgeon and prosthodontist is must for better facial esthetics and oral functions.
CONCLUSION
Guided eruption of impacted teeth with coordinated multidisciplinary management is essential for treatment of patients with multiple impactions. An idiopathic (unknown cause) cause of multiple impacted teeth could only be postulated as possible diagnosis in these case scenarios since the authors were unable to put forward a metabolic or syndromic pathogenesis.
- Kumar GS (2009) Orban’s Oral Histology and Embryology. 12th ed. Mosby, India.
- Lindauer SJ, Rubenstein LK, Hang WM, Andersen WC, Isaacson RJ (1992) Canine impaction identified early with panoramic radiographs. J Am Dent Assoc 123(3): 91-97.
- Becker A, Lustmann J, Shteyer A (1997) Cleidocranial dysplasia: Part 1-General principles of the orthodontic and surgical treatment modality. Am J Orthod Dentofacial Orthop 111(1): 28-33.
- Grover PS, Lorton L (1985) The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol 59(4): 420-425.
- Kramer RM, Williams AC (1970) The incidence of impacted teeth: A survey at Harlem Hospital. Oral Surge Oral Med Oral Pathol 29(2): 237-241.
- Cooper SC, Flaitz CM, Johnston DA, Lee B, Hecht JT (2001) A natural history of cleidocranial dysplasia. Am J Med Genet 104(1): 1-6.
- Kirson LE, Scheiber RE, Tomaro AJ (1982) Multiple impacted teeth in cleidocranial dysostosis. Oral Surg Oral Med Oral Pathol 54(5): 604.
- Sharma A (2001) A rare non-syndrome case of concomitant multiple supernumerary teeth and partial anodontia. J Clin Pediatr Dent 25(2): 167-169.
- Yalcin S, Gurbuzer B (1993) Multiple impacted teeth in the maxilla. Oral Surg Oral Med Oral Pathol 76(1):130
- Sivakumar A, Valiathan A, Gandhi S, Mohandas AA (2007) Idiopathic failure of eruption of multiple permanent teeth: Report of 2 adults with a highlight on molecular biology. Am J Orthod Dentofacial Orthop 132(5): 687-692.
- Chodirker BN, Chudley AE, Toffler MA, Reed MH, Opitz JM, et al. (1986) Zimmerman‐Laband syndrome and profound mental retardation. Am J Med Genet 25(3): 543-547.
- Babu V, Nagesh KS, Diwakar NR (1998) A rare case of hereditary multiple impacted normal and supernumerary teeth. J Clin Pediatr Dent 23(1): 59-61.
- Sujatha G, Sivapathasundharam B, Sivakumar G, Nalinkumar S, Ramasamy M, et al. (2012) Idiopathic multiple impacted unerupted teeth: Case report and discussion. J Oral Maxillofacial Pathol 16(1): 125.
-
 Table 1
Table 1 -
Table 2









QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Pathology and Toxicology Research
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Advance Research on Alzheimers and Parkinsons Disease
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)



