705
Views & Citations10
Likes & Shares
Blood cancer is disease which keeps the separation of platelets amid hematopoiesis, prompting strange cell development. Very lately, improved chemotherapy and hematopoietic undeveloped cell transplantation have upgraded the treatment of blood cancer. This investigation broke down the contrasts between three treatment bunches in steady consideration necessities of patients with blood malignant growth at a college clinic, especially in connection to remedial purposes in such patients.
INTRODUCTION
Blood cancer is a malignant disease that prevents the differentiation of blood cells during hematopoiesis, leading to abnormal cell growth [1]. Despite the steady worldwide growth in its prevalence [2], recently, improved chemotherapy and hematopoietic stem cell transplantation have enhanced the treatment of blood cancer [1]. However, many patients experience adverse physical and mental effects during diagnosis and treatment, in addition to physical symptoms such as pain, fatigue, and lack of appetite, leading to a decline in their physical and social functioning [3-6]. These adverse reactions are a result of both the disease manifestation and treatments, which are different from the treatments of solid cancers [7,8]. The quality of life may decrease after hematopoietic stem cell transplantation [9,10]. Thus, the well-being of patients with blood cancer must be monitored during treatment [11]. Therefore, while the needs of patients need to be identified to provide supportive patient care, not many studies have assessed the needs of patients based on the nature of the disease and treatment.
This study analyzed the differences between three treatment groups in supportive care requirements of patients with blood cancer at a university hospital, particularly in relation to therapeutic purposes in such patients.
METHODS
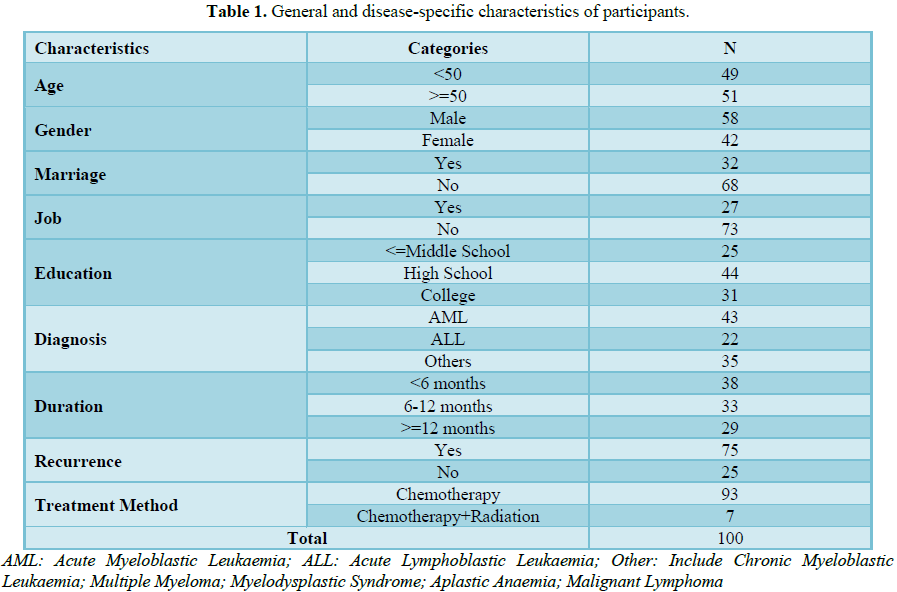
The study was conducted from February 2016 to May 2016. Subjects were 100 patients diagnosed with blood cancer at K Hospital, a general hospital in Daegu, were hospitalized for chemotherapy or outpatient treatment and knew disease diagnosed and could communicated with interviewers. The institutional review board of K national university hospital approved the study (no. 2016-02-020). All participants provided written informed consent prior to starting the survey. Subjects were excluded if they didn’t know their own disease or couldn’t communicate with interviewers. The questionnaire used in this study consisted of 13 questions regarding the general and disease characteristics of the patients and 59 questions regarding supportive care needs [12] that were validated in other Korean study [13]. Some disease related data were obtained using hospital information system. The patients were divided into three groups, the chemo radiation at first diagnosis (1st Dx) group, the consolidation and maintenance treatment (CM) group and chemo radiation before hematopoietic stem cell transplantation (HST) group. To analyze the differences among treatment purposes, p values were calculated in the analysis of single variation when determining calibration intervals. All statistical tests were performed using SPSS 22.0, and the statistical significance level for the hypothesis test was 0.05.
RESULTS AND DISCUSSION
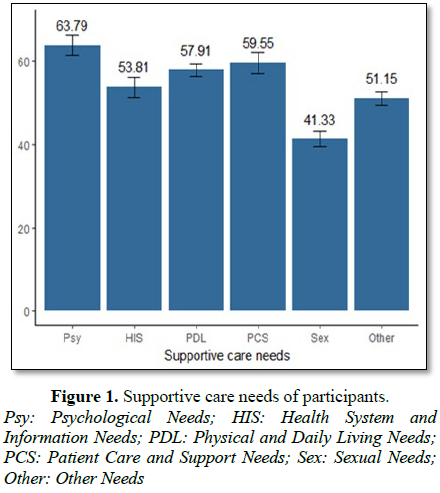
The inter area scores of supportive care needs are shown in Figure 1. The scores for psychological, health system and information, physical and daily living, patient care and support, sexual, and other needs were 63.79, 53.81, 57.91, 59.55, 41.33 and 51.15 points, respectively.
The results of analyses of supportive care needs in accordance with therapeutic purposes are presented in Table 2. Multivariate analysis was performed with adjustments for age, sex, marital status, occupational status, education, diagnosis, duration of treatment, purposes of treatment and recurrence (p<0.2 in the univariate analysis). As observed in the univariate analysis, psychological, health system and information, and patient care and support needs varied depending on the therapeutic purpose (p<0.001) and physical and daily living, sexual, and other needs. The score for psychological needs was higher in patients in the consolidation and maintenance treatment (CM) group than those in the chemo radiation at first diagnosis (1st Dx) and chemo radiation before hematopoietic cell (HST) groups (p<0.001). The health system and information needs score was the highest in the 1st Dx group, followed by the HST and CM groups (p<0.001). The patient care and support needs score was the highest in the HST group, followed by the CM and 1st Dx groups (p<0.001).
Although these findings revealed that psychological needs were the highest in these patients, there were differences in the need for care depending on the study participant and disease type. Jung and Yi [6] reported high scores for health systems and information needs in patients with blood tumor and Hwang et al. [14] also reported the same result in breast cancer. Other studies on patients with blood tumors [15,16] also revealed high psychological and physical needs. In this study, the health system and information needs of patients receiving treatment after the first diagnosis were the highest. In contrast to our study, more than half of the subjects in the study by Jung and Yi [6] had been diagnosed at <6 months before enrollment; thus, the health system and information needs were likely to be higher.
In this study, we analysed the supportive care needs of patients with blood cancer who underwent treatment for a long period, which differs from the treatment of other solid malignancies. In the 1st Dx group, the patients had the highest need for supportive care in the health system information area because of the intensive treatment from the time of diagnosis, without having the time for psychological preparations due to the nature of the treatment for hematological malignancies. Patients may not have sufficient time for communication with the medical staff, and the medical staffs often fail to understand the exact nature of information that the patients desire [17]. Therefore, early identification of patients’ needs as well as sufficient explanation of the disease and treatment process is important.
The need for psychological care was the highest in the CM group. Increased energy expenditure continued anorexia and destroyed fat deposits during cancer chemotherapy increase fatigue, in addition to a variety of physiological, psychological, and social factors that contribute to the development of fatigue in patients undergoing chemotherapy [5]. In addition, because of the nature of hematological malignancies, the prognosis of the treatment remains uncertain. Therefore, during long-term chemotherapy, patients experience a variety of emotional changes, such as fear, anxiety and hopelessness [18]. Psychological needs tend to increase during multiple chemotherapy regimens after induction therapy.
Patient care and support needs were the highest in the HST group because these patients remain isolated from family and relatives and are socially marginalized following transplantation [19]. Because sensory stimuli are reduced or deprived, psychosocial problems arise, and patients face many physical and mental risks following transplantation [7]. Furthermore, the need for direct care could be heightened due to long-term illness and treatment effects.
CONCLUSION
The purpose of this study was to investigate the supportive care needs of patients with hematological malignancies who were treated with chemotherapy. During long-term anticancer chemotherapy, there were significant differences in supportive care needs according to the treatment goals. To provide patient-oriented medical services, supportive care needs should be assessed and appropriate services should be provided.
1. The Korean Society of Hematology (2011) Hematology. Panmuneducation: Seoul.
2. National Institutes of Health (2017) NIH Senior Health. Available at http://nihseniorhealth.gov (Accessed on 15 January, 2017).
3. Johnsen AT, Tholstrup D, Petersen MA, Pedersen L, Groenvold M (2009) Health related quality of life in a nationally representative sample of hematological patients. Eur J Hematol 83: 139-148.
4. Redaelli A, Stephens JM, Brandt S, Botteman MF, Pashos CL (2004) Short- and long-term effects of acute myeloid leukemia on patient health-related quality of life. Cancer Treat Rev 30: 103-117.
5. Son H, Kim S, Sohn S (2007) Relationship between fatigue and depression in patients with hemato-malignancy receiving chemotherapy. J Korean Oncol Nurs 7: 14-25.
6. Jung AR, Yi MS (2011) Predictive factors of supportive care needs in patients with hematologic malignancy. Korean J Adult Nurs 23: 460-471.
7. DeMarinis V, Barsky A, Antin J, Chang G (2009) Health psychology and distress after haematopoietic stem cell transplantation. Eur J Cancer Care 18: 57-63.
8. Howell DA, Shellens R, Roman E, Garry AC, Patmore R, et al. (2011) Haematological malignancy: Are patients appropriately referred for specialist palliative and hospice care? A systematic review and meta-analysis of published data. Palliat Med 25: 630-641.
9. Song BY, Kang HR, Kim KS (2008) Quality of life in patients with hematopoietic stem cell transplant. J Korean Oncol Nurs 8: 40-49.
10. Bok J, Sohng K, Park H (2005) Quality of life and family burden in hemopoietic stem cell transplantation recipients. J Korean Oncol Nurs 5: 136-145.
11. Fincham L, Copp G, Caldwell K, Jones L, Tookman A (2005) Supportive care: Experiences of cancer patients. Eur J Oncol Nurs 9: 258-268.
12. Bonevski B, Sanson‐Fisher R, Girgis A, Burton L, Cook P, et al. (2000) Evaluation of an instrument to assess the needs of patients with cancer. Cancer 88: 217-225.
13. Ham YH (2009) Supportive care needs of patients with advanced lung cancer [dissertation]. Sungkyunkwan University, Korea.
14. Hwang SY, Kim SI, Park BW (2004) The supportive care needs of breast cancer patients. J Korean Surg Soc 67: 265-273.
15. Boyes AW, Clinton-McHarg T, Waller AE, Steele A, D’Este CA, et al. (2015) Prevalence and correlates of the unmet supportive care needs of individuals diagnosed with a haematological malignancy. Acta Oncol 54: 507-514.
16. Molassiotis A, Wilson B, Blair S, Howe T, Cavet J (2011) Unmet supportive care needs, psychological well‐being and quality of life in patients living with multiple myeloma and their partners. Psychooncology 20: 88-97.
17. Brown V, Sitzia J, Oakley C, Hughes J, Hannon H, et al. (2001) The development and evaluation of an instrument to assess the adverse effect of cytotoxic chemotherapy. NHS Executive South East Research Project Grant Cheme: UK.
18. Mishel MH (1988) Uncertainty in illness. J Nurs Scholarsh 20: 225-232.
19. Kang YA, Yi M (2009) Ethnography on isolation unit for hematopoietic stem cell transplantation: Focusing on patients. J Korean Oncol Nurs 9: 31-42.
-
 Table 1
Table 1 -
Table 2

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Pathology and Toxicology Research
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Rheumatology Research (ISSN:2641-6999)


