787
Views & Citations10
Likes & Shares
Brain cancer is classified based on the World Health Organization's (WHO) histological classification system, which focuses on the tumor's biological behavior (ICD-10-CM Diagnosis Code C71). Brain cancer is one of the most aggressive and difficult-to-treat malignancies. Primary malignant brain tumors are rare, accounting for 1.4% of new cancer diagnoses in the United States and 2.7% of deaths due to cancer.
Keywords: Young women, Brain tumor, Ukraine
INTRODUCTION
Primary brain cancer is the third most common
cause of cancer deaths in adults aged 15 to 34 [1-4]. American Brain Tumor
Age-standardized incidence rate (Ukrainian standard) of brain tumor among women
in Lviv region due to Bulletin of National Cancer Registry of Ukraine
(2016-2017) contains 5.5 per 100,000 [5]. In Ukraine age-standardized incidence
rate (Ukrainian standard) is smaller and is 4.2 per 100,000. In 2016 brain
cancer among females in Ukraine was second only to deaths (11.5%) in the age
group of 18-29 years.
Understanding the epidemiology of such
tumors, as well as the underlying genetics, will help to tackle this
devastating disease. Environmental factors may also contribute to the increased
risk of brain tumor in young people. The role of carcinogens in the etiology of
brain tumors is controversial, but limited studies do demonstrate factors that
are prevalent in the youth that includes smoking and pollution [6,7].
Primary brain cancer can be categorized into
2 types: gliomas and non-gliomas. Malignant gliomas originate in the glial
cells of the CNS and are the more common and more lethal form of brain
malignancies. Non-gliomas do not originate in the glial cells of the CNS. These
tumors develop in other parts of the brain. Some examples of non-gliomas
include meningiomas and medulloblastomas [7,8].
Brain cancer does not have a specific staging
system that is capable of accurately predicting the cancer's development and
likely outcome. The TNM system is not an appropriate tool for brain cancer because
most brain and spine cancers are unable to spread to other organs
(metastasize).
Despite a lack of progress in the clinic,
research on this group of conditions is advancing steadily and treatments with
the potential to transform the field are on the horizon [9-11].
AIM OF OUR STUDY
It was to assess the epidemiology
characteristics in young women with brain tumor from Lviv region (Ukraine)
during 1992-2018.
We used the Cancer Register of our region,
which contains the largest aggregation of population-based data on the
incidence of primary central nervous system tumors in the Lviv region (West
Ukraine) to describe these tumors.
The following key variables were extracted
and utilized: year of diagnosis, age at diagnosis, registry, discrete at
diagnosis, region at diagnosis, diagnostic confirmation, reporting source and
type of treatments.
RESULTS
We obtained the latest available
population-based data on all newly diagnosed primary brain tumors from the Lviv
Cancer Register (West of Ukraine) in 1992-2018. We studied cohort of young
women from 20 districts of Lviv region and Lviv town during these years.
According to the Statistical Office on April 2018 population was 2,526,500
persons, including 1,321,600 women (52.3%) in Lviv region (West Ukraine) [12].
Every year in the Lviv region about 5-11 young women of different ages are
found to have confirmed brain tumor. Age of patients ranged from 18 to 35 years
(median of 28.2 ± 6.4 years).
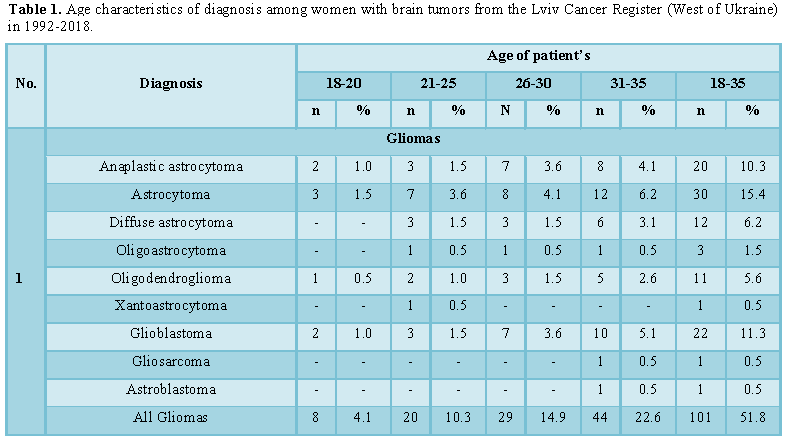
A total of 195 (Table 1) primary brain tumor patients were selected from the Lviv
Cancer Register database. In which the most common cases were gliomas - 101
(51.8%). In our study were two main types of glioma: astrocytoma (30 cases
-15.4%) and oligodendroglioma (12 cases - 6.2%). The most common types of brain
tumor in young women were anaplastic astrocytoma (astrocytoma, grade 3) - 20
(10.3%) cases and glioblastoma (astrocytoma, grade 4) - 22 (11.3%) cases.
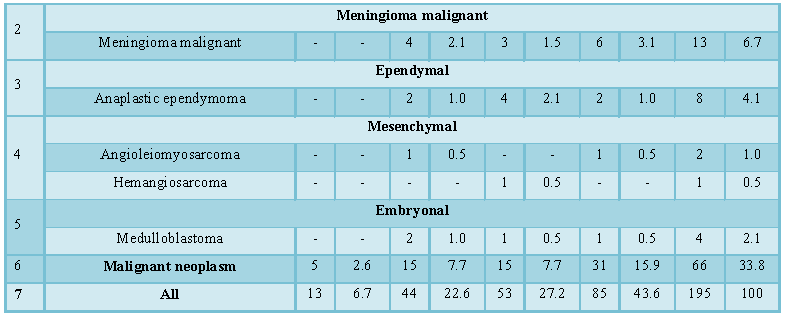
Anaplastic ependymoma met in 8 (4.1%) cases. Malignant neoplasm - 66 (33.8%)
ranks second among brain tumors in women of young age. The third place was
taken by meningioma malignant -13 (6.7%). Mesenchymal malignant, a group of
rare tumors that includes angioleiomyosarcoma and hemangiosarcoma, comprises
1.5% of all brain tumors.
With age, the number of pathology increased.
The incidence rate for malignant brain tumors in aged 18-20 – 13 (6.7%)
cases is significant less than 31-35
years old – 85 (43.6%), p<0.05. In each age group’s there was an increase in
the number of all brain tumors with age. There was no difference (p>0.05)
almost among groups aged 21-25 (44 cases – 22.6%) and 26-30 (53 cases – 27.2%).
The amount of glioblastoma significant
increased (p<0.05) with the age requirement of 2 (1%) cases at the age of
18-20 years to 10 (5.1%) cases aged 31-35.
Independently of age dominated glial tumors
among young women with brain tumors, especially at the age of 26-30 years – 29
(14.9%) cases and 44 (22.6%) in group 31-35 aged. The significant lowest age of
the onset of glial tumors (p<0.05) were in group 18-20 aged – 8 (4.1%) cases
than in group 31-35 aged.
Medulloblastoma
was relatively rare and account for 2.1% (4 cases) of all primary brain tumors
which coincides with the data [13]. At the age of 21-25 years were diagnosed
two cases (1%) of this pathology in women from Lviv region.
Epidemiological data among 195 female
patients with brain tumor from Lviv region during 1992-2018 showed that there
were two cases (1%) compared with other tumor. A woman В. 31 years old was
diagnosed with rhabdomyosarcoma of the lung for which pneumoectomy was
performed. Nine months later suspected anaplastic astrocytoma. Patient refused
from treatment and dead one year after diagnosis. A patient F at the age of 34
years found leukemia and malignant neoplasm of brain simultaneously. Woman
received palliative chemotherapy due to leukemia. The patient died 3 months
after the diagnosis was established.
Gliomas can be low grade (slow growing) or
high grade (fast growing). Doctors used the grade to decide which treatment
they need. The position of the tumor was also very important. Primary brain
tumors were treated using a multipronged approach that can involve surgery,
radiotherapy or chemotherapy (Table 2).
Among 195 women 34 (17.4%) patients were refused from treatment. The rest of
161 (82.6%) young women received different treatment (Table 2): radical treatment – 77 (39.5%), palliative – 84 (43.1%).
For brain tumors, surgery 44 (22.6%) was the
first choice of treatment to help relieve symptoms and increase patient
survival. Treatment began with maximal surgical removal of the tumor. When
surgery could not be done, then chemotherapy with or without radiation therapy
were used. The addition of radiation to the entire neuraxis and chemotherapy
helped improve survival.
Only radiation therapy was applied in 7
(3.6%) women – 3 radical and 4 palliative cases. Only chemotherapy drugs were
used in 6 (3.1%) women. Surgery with chemotherapy without radiation therapy was
observed in 5 (2.6%) patients.
In most cases treatment was include some
combination of surgery, radiation therapy and chemotherapy. Radiation therapy
with chemotherapy (Table 2) were
given in 8 (4.1%), radiation with surgery – in 5 (2.6%) cases. Radiation
therapy with chemotherapy and surgery were used in 2 (1%) cases, radiation
therapy with surgery and chemotherapy – 3 (1.5%) cases.
Radiation therapy was used after surgery or
chemotherapy in 76 (39%) cases. In 5 (2.6%) cases radiation therapy was given
after surgery and chemotherapy.
In our study combinations of treatments with
radiation therapy was used for treatment brain tumor in 140 (71.8%) cases.
CONCLUSION
1. This
retrospective study evaluated in 195 female patients with brain tumor aged
18-35 years (median 28.2 ± 6.4) from Lviv region (West Ukraine) who were diagnosed
and followed-up over a period of 27 years (1992-2018) in the Cancer Register of
Lviv Oncologic Regional Treatment and Diagnostic Center.
2. The
incidence rate for malignant brain tumors in aged 18-20 – 13 (6.7%) cases is
significant less than 31-35 years old – 85 (43.6%), p<0.05.
3. The
most common cases among ill women of young age from Lviv region were gliomas –
101 (51.8%). Malignant neoplasm – 66 (33.8%) ranks second among brain tumors of
these patients.
4.
Among 195 women 34 (17.4%) patients were
refused from treatment. The rest of 161 (82.6%) young women received different
treatment in our study combinations of treatments with radiation therapy were
used for treatment brain tumor in 140 (71.8%) cases.
1.
Siegel RL, Miller KD, Jemal A (2018) Cancer
statistics, 2018. CA Cancer J Clin 68: 7-30.
2.
National Brain Tumor Society (NBTS) (2018) Quick Brain
Tumor Facts. Available at: http://braintumor.org/brain-tumor-information/brain-tumor-facts/
3.
Tish S, Habboub G, Jones J, Ostrom QT, Kruchko C, et
al (2019) The epidemiology of central and extraventricular neurocytoma in the
United States between 2006 and 2014. J Neuro-Oncol 2019: 1-5.
4.
Ostrom QT, Gittleman H, de Blank PM, Finlay JL, Gurney
JG, et al. (2015) Adolescent and young adult primary brain and central nervous
system tumors diagnosed in the United States in 2008-2012. Neuro-Oncology 18:
i1-i50.
5.
http://www.ncru.inf.ua/publications/index.htm
6.
Zhang AS, Ostrom QT, Kruchko C, Rogers L, Peereboom DM
(2017) Complete prevalence of malignant primary brain tumors registry data in
the United States compared with other common cancers, 2010. Neuro-Oncology 19:
726-735.
7.
Wrensch M, Minn Y, Chew T, Bondy M, Berger MS (2002)
Epidemiology of primary brain tumors: Current concepts and review of the
literature. Neuro-Oncology 4: 278-299.
8.
Song Y, Kang X, Cao G, Li Y, Zhou X, et al. (2016)
Clinical characteristics and prognostic factors of brain central neurocytoma.
Oncotarget 7: 76291-76297.
9.
Rozumenko V, Rozumenko A (2016) Endoscope-assisted
surgery of deep-seated brain tumors. Ukrainian Neurosurg J 25: 5-8.
10.
Ostrom QT, Gittleman H, Kruchko C, Barnholtz-Sloan JS
(2018) Primary brain and other central nervous system tumors in Appalachia:
Regional differences in incidence, mortality and survival. J Neurooncol 142:
27-38.
11.
Furuse M, Nonoguchi N, Yamada K, Shiga T, Combes JD,
et al. (2019) Radiological diagnosis of brain radiation necrosis after cranial
irradiation for brain tumor: A systematic review. Radiat Oncol 14: 14-28.
12.
http://lv.ukrstat.gov.ua/ukr/
13.
Faried A, Pribadi MA, Sumargo S, Arifin MZ, Hernowo BS
(2016) Adult medulloblastoma: A rare case report and literature review. Surg
Neurol Int 7: S481-484.
-
 Table 1
Table 1 -
Table 2
-
Table 3

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Journal of Ageing and Restorative Medicine (ISSN:2637-7403)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Advance Research on Alzheimers and Parkinsons Disease


