656
Views & Citations10
Likes & Shares
Background: Deaf mutism can
affect the development of speech, social, cognitive and academic abilities.
Adolescence is the stage of life with rapid developmental changes, the concept
of quality of life (QoL) is important to understand for adolescents who
experience hearing loss because of the importance of communication and social
participation in everyday life. Bengkala village in Bali, Indonesia, has a
population of deaf mutism of 44 individuals in 3.032 inhabitants or around
1.4%, is caused by recessive gene mutations at the DFNB3 locus. The aim of this
study is to find out whether there are differences in the QoL of deaf mutism
adolescents in Bengkala and deaf school as control.
Method: This study is an
observational analytic study using cross-sectional design. The subjects in this
study were deaf mutism adolescents in Bengkala and who attended deaf school as
many as 22 people. The Youth Quality of Life Instrument – Deaf and Hard of
Hearing (YQOL-DHH) questionnaire was filled in with three domains, namely
self-acceptance, stigma and participation.
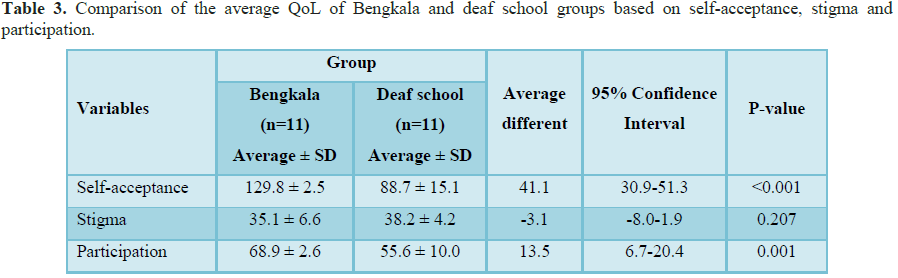
Results: From the results
of the independent t-test, the average QoL based on self-acceptance in Bengkala
was 129.8 ± 2.5 while in deaf school was 88.7 ± 15.1. The mean QoL based on
stigma in Bengkala was 35.1 ± 6.6 while in deaf school was 38.2 ± 4.2. The mean
QoL based on participation in Bengkala was 68.9 ± 2.6 while in deaf school was
55.6 ± 10.0.
Conclusion: The quality of
life of adolescents with deaf mutism in Bengkala village and deaf school based
on of self-acceptance and participation found significant differences with
significance values, while stigma was not statistically significant.
INTRODUCTION
Bengkala village is
one of the villages in Kubutambahan district, Buleleng regency, Bali,
Indonesia, has a population of deaf people with as many as 44 individuals in
3,032 inhabitants or around 1.4%. They are referred to as kolok, which means they cannot hear in Balinese. Winata et al. [5]
using the DNA (Deoxyribonucleic acid) Short Tandem Repeat method, found that
there was a recessive gene mutation at the DFNB3 locus on chromosome 17.
Therefore the type of deafness that is owned by Bengkala villagers is an
autosomal recessive non-syndromal hearing disorder. The results of the study
also estimated that DFNB3 had appeared in the gene pool of Bengkala villagers
from 150-300 years ago. According to Lestari and Luthfiana [6], the community
in Bengkala has created social cultural inclusion for deaf mutism as part
of a community that
also has a role in
Adolescence is a
stage of life with rapid developmental changes, but little is known about how
these changes affect the quality of life (QoL) of adolescents with hearing
loss. Patrick et al. [7] from the University of Washington developed an
instrument Youth Quality of Life Instrument-Deaf and Hard of Hearing (YQOL-DHH)
which has been validated and widely publicized. This questionnaire consists of
3 dimensions that reflect the important aspects of the lives of adolescents
with hearing loss, namely self-acceptance, participation and perceived stigma.
Measuring how their QoL can provide children, parents, and physicians important
information that can help guide individual and social choices to optimize
subjective well-being [8]. Research comparing the community of deaf teenagers
has never been done. Therefore the authors are interested in knowing whether
there are differences in the quality of life of deaf mutism adolescents in
Bengkala Village compared to deaf school students.
METHOD
This research method
is analytical research with cross sectional study approach. Research location
in Bengkala village and one of deaf school in Bali, Indonesia. Pure tone
audiometry is performed on all deaf mutism to find out the hearing threshold.
The study population was deaf mutism aged 11-18 years who lived in Bengkala and
attended deaf school during the study period in December 2018 to January 2019.
Inclusion criteria are deaf mutism aged 11-18 years, living in Bengkala and
attending deaf school, willing to complete the questionnaire completely.
Exclusion criteria are patients with other syndromal disorders such as Down's
syndrome, Usher's syndrome and others. Data collected were analyzed
statistically using SPSS version 2.4 for Windows computer software. The
descriptive analysis of the study included the presentation of the results
descriptively using numerical and categorical data. Normality test using
Shapiro-Wilk test was obtained, the data were normally distributed, then
continued with independent-t test.
RESULTS
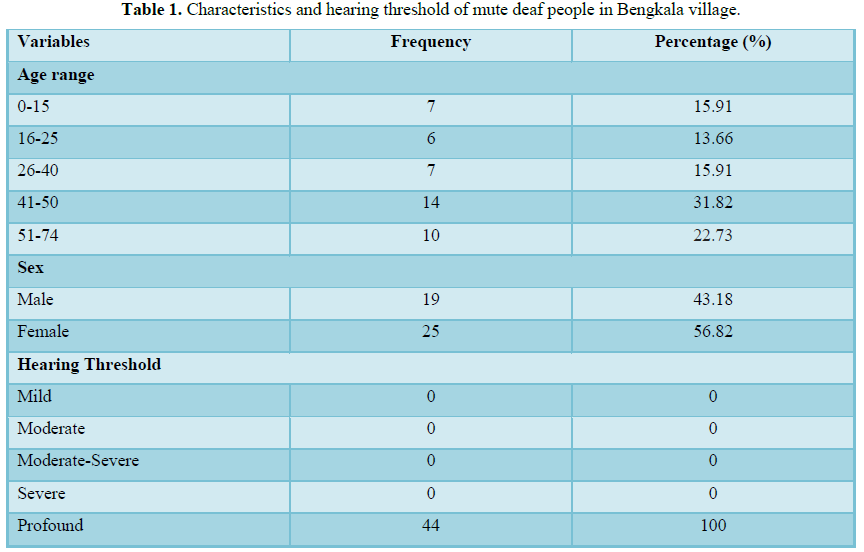
Deaf mutism in
Bengkala village numbered 44 people and pure tone audiometry was performing to
find out the hearing threshold in 43 people. One person was under 7 years old
and performed Brainstem Evoked Response Audiometry (BERA) for diagnostic (Table 1).
DISCUSSION
In this study, deaf
mutism in Bengkala Village were 44 people, 19 male (43.18%) and 25 female
(56.82%), the majority of hearing impaired people were 41-50 years old as many
as 14 people (31.82%), while the lowest is in 2 age groups, 16-25 years are 6
people (13.66%). The hearing threshold of all deaf population is profound
(100%).
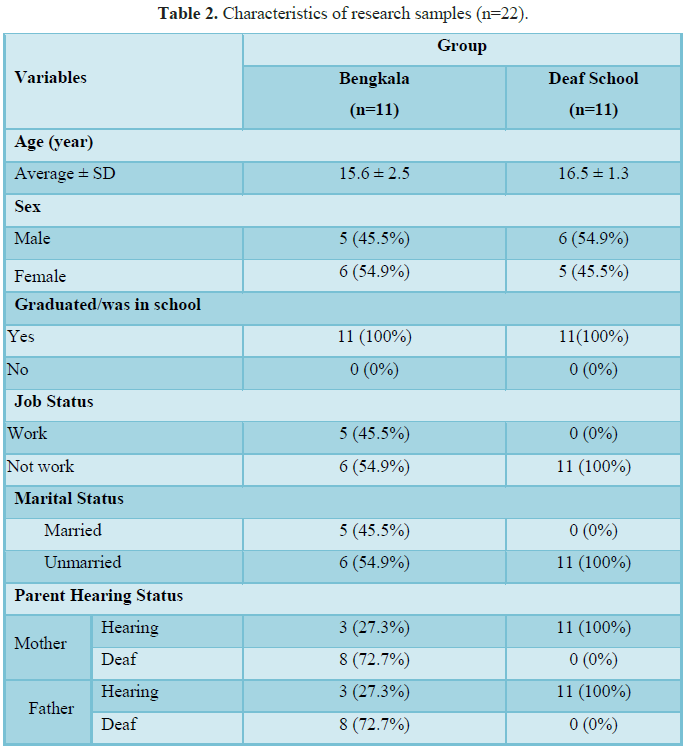
Characteristics of research sample
Samples in Bengkala
numbered 11 people aged 12-18 years, male as much as 45.5% and female 54.5%.
While the sample in deaf school was 11 people with ages ranging from 15-18
years, male were 54.5% and female were 45.5%. Based on the level of education,
all samples in Bengkala were in school, i.e., 3 people were attending an
inclusive elementary school in Bengkala and 8 were elementary school graduates
and did not continue to the next level due to various reasons. All samples at
deaf school are attending school at the junior high school and high school. The
research in the United States about the QoL of adolescents with severe to
profound sensorineural hearing loss followed by adolescents as many as 157
people aged 11-18 years (mean age 14.1 years) with male gender as much as 47.7%
and female 52.3%. All research subjects are currently taking various levels of
education both in public schools, inclusive schools and deaf schools.
Samples in Bengkala
were 5 people who had worked with various types of work, including as
photographers, farmers, and laborers, as well as 6 people who did not work,
namely 2 housewives, 3 people were in school and 1 person had not worked. All
samples in deaf school did not work because they were still in school. The
marital status of research subjects in Bengkala was obtained by 5 married
people and 6 unmarried people, while in deaf school all were not married.
Research by Borujeni et al. [8] in Iran about the QoL of deaf mutism
adolescents followed by non-worker and unmarried adolescents who are still
pursuing education in public schools, inclusive schools and deaf schools.
Based on the hearing
status of the parents of the research subjects, in Bengkala it was obtained
from the mother or from the father's side as many as 3 people could hear and 8
people did not hear, while in the deaf school from the mother or other parties
(100%) could hear. The hearing statuses of parents of subjects are parents who
heard as much as 84.7%, one parent who was not seen as much as 5.1% and both
people who did not hear as much as 9.0% and 2 samples did not know the hearing
status of their parents. Winata et al. [5] in Bengkala found that there is a
recessive gene mutation that is needed for the birth of individuals with
hearing loss. This is due to local endogamy carried out by deaf mutism in
Bengkala from generation to generation.
Differences in mean QoL based on self-acceptance
Accepting
self-condition, especially physical condition and being able to use it
effectively is one form of adolescence adjustments at the stage of human
development. Hurlock [9] states self-acceptance as a level at which a person
has considered his characteristics feels capable and is willing to live with those
characteristics.
Ebahimi et al. [10]
states that the birth of a child with deafness is a stressful and unpredictable
life experience for parents. In general, around 90% of children with deafness
are born from normal hearing parents, this is consistent with this study in the
deaf school subject group, which is 100% having normal hearing parents.
Khotimah [11] states that if parents, especially mothers, accept the condition
of the child, it will be able to help in care and will support children's
development. The results of her research show that the picture of acceptance
shown by the subject, namely the existence of realistic expectations of the
situation, confidence in his standards, has a calculation of limitations on
himself, aware of his own assets and realize the shortcomings. Wasito et al.
[12] found that people with deaf mutism from deaf parents also showed
relatively better social maturity than deaf people from hearing parents. Local
endogamy carried out by deaf mutism in Bengkala caused most parents of deaf
mutism adolescents also be deaf and mute. Parents consciously choose couples
who are both deaf and have prepared themselves and surrender/accept if someday
will give birth to deaf descendants as well.
In Bengkala there is
an inclusive school that aims to provide opportunities for deaf mutism students
to learn about diverse friends, not only fellow students, and have the
potential to provide social support so that social competencies including
adaptability will develop and will later make them ready to be involved on
normal activities in the wider community[13]. This is in accordance with the
opinion of Fellinger [14], where deaf mutism children have lower psychosocial
problems when in inclusive schools compared to when in deaf school. This
opinion is also supported by research conducted by Alwis [15] that when deaf
mutism students study in inclusion schools, they have good adaptation because
their peers and teachers interact well with them. While when at deaf school,
deaf mutism students do not interact with hearing students during the learning
process at school because in deaf school students with special needs learn
together with students with special needs who have the same specificity as him.
In addition to the
conditions previously explained, the community of Bengkala has a unique thing,
namely the belief of Bhatara Bongol (Deaf God) as one form of public perception
about deafness experienced by local residents. This belief has been preserved
for hundreds of years and is followed by historical relics that have been
discovered and studied [16]. The existence of these beliefs also creates a
sense of accepting/surrender to the condition of their deafness that has been
experienced for generations.
Difference in mean QoL based on stigma
Donaldson [17] said
that individuals who are stigmatized may have their own beliefs about how other
people's judgments or feelings towards the condition of stigma exist in
themselves and then internalize those judgments. So that it can be said that
when someone experiences interaction or negative treatment from others, it will
form perceived stigma, meaning that individuals form their own perceptions
about how other people's judgments or feelings toward him or her are affected
by stigma and internalize that stigma towards him.
Hurlock [9] suggests
one condition that causes adolescents not to get social acceptance is the lack
of maturity, especially in controlling emotions, calmness, confidence and
wisdom. In general, these conditions eventually make deaf mutism will look for
deaf mutism fellow also in a closer relationship. This condition also occurs
both in Bengkala and in the other areas, including in deaf school that have
dormitory facilities. This is also consistent with the statement by Santrock
[18], that individuals from minorities, in this case deaf mutism, consider
relations with peers who also come from minorities will give feelings of
brothers who are very important and reduce isolation in themselves the
individual.
Batten et al. [19]
stated that deaf mutism adolescents may be delayed in communication and social
skills due to limited communication experience from the beginning. The
experience of communication as early as possible is very important, because
without it dumb deaf teenagers may struggle to develop theories that are
appropriate to the age of thought and social competence, which in turn can
negatively impact the development of communication and maintain their
self-stigma thereby reducing further opportunities communication and social
skills.
Differences in mean QoL based on participation
Leary [20] states
that social acceptance means that there is a signal from other people who want
to include someone to join a relationship or social group. Social acceptance
occurs starting from tolerating the presence of others to actively wanting
someone to be a partner in a relationship. Social acceptance is one of the
factors that influence a person's participation. Participation is the active
involvement of someone in responding to activities and supporting the achievement
of goals and being responsible for their involvement.
Youth groups in Bali
have their own place in the social environment. In each village consisting of
several banjar (groups), they have an association called Sekaa Teruna Teruni
(STT) and consist of unmarried teenagers. Research by Kurniati et al. [21] in
Bengkala regarding the understanding and acceptance of STT members towards deaf
mutism stating that all STT members both men and women received well the
presence of deaf mutism in their area. Their form of acceptance is by including
deaf mutism adolescents in STT, making friends, and involving them in several
activities in their village. The activity that they often do together is during
mutual cooperation in preparing religious ceremonies at the temple. They stated
that they were not ashamed to be friends with the deaf mutism and highly valued
them as individuals who were diligent in their work. Deaf mutism adolescents
are given preferential treatment in the form of discharge from all obligations
such as organizational contributions.
An environment that
can accept deaf mutism will make individuals easily make adjustments to other
people and have great motivation for their future. Conversely, if the
environment cannot accept it, what will happen is that the individual becomes
isolated and closes himself in his social environment. This environmental
influence causes deaf mutism to be difficult to do social interaction with
other people either personally or in groups, making individuals tend to be
happier to get along with their communities, namely deaf mute communities [19].
The local wisdom of
Balinese culture such as the Tri Hita Karana concept can be adapted in today's
social life, especially in the area/environment with a diverse composition of
society, including people with disabilities; in this case the person is deaf
and mute. The concept of Tri Hita Karana as the basis for gaining happiness in
life which is essentially a balanced attitude between worshiping God and
serving others and developing compassion for the environment. In this context
the emphasis is on human relations that have been well implemented in Bengkala,
such as the spirit to mingle, communicate and cooperate with all citizens, both
normal hearing and deaf mutism residents. The community in Bengkala has created
social cultural inclusion for deaf mutism as part of a community that also has
a role in community life [6]. They are accepted in their families and in the
community and are given full rights and responsibilities in the village. They
participate fully and are active in all areas and lives of the community. This
social life in Bengkala also reflects the implementation of Pancasila as the
basis of the Indonesian state, especially the principle of just and civilized
humanity and social justice for all the people of Indonesia.
CONCLUSION
The QoL between deaf
mutism adolescents in Bengkala Village and deaf school based on self-acceptance
and participation statistically found differences, while the QoL based on
stigma was not statistically different.
ACKNOWLEDGEMENT
Author(s) received no
specific funding for this work.
1.
Steer CD, Bolton P, Golding J (2015) Preconception and
prenatal environmental factors associated with communication impairments in 9
year old children using an exposome-wide approach. PLoS One 10: 23-25.
2.
Sivakumaran TA, Husami A, Kissel D, Zhang W, Keddache
M, et al. (2013) Performance evaluation of the next generation sequencing
approach for molecular diagnosis of hereditary hearing loss. Otolaryngol Head
Neck Surg 146: 1007-1016.
3.
Gurtler N (2008) Hereditary hearing impairment. In:
Lalwani AK; Current Diagnosis and Treatment in Otolaryngology Head and Neck
Surgery. USA: The McGraw Hill, pp: 697-704.
4.
Soetjipto D (2016) Komite Nasional Penanggulangan
Gangguan Pendengaran dan Ketulian. Available at: http://komnaspgpkt.blogspot.com/
5.
Winata S, Arhya IN, Moeljopawiro S, Hinnant JT, Liang
Y, et al. (1995) Congenital non-syndromal autosomal recessive deafness in
Bengkala, an isolated Balinese village. J Med Genet 32: 336-343.
6.
Lestari W, Luthfiana Y (2013) Orang kolok dan orang
inget: Studi kasus tentang inklusi sosial difabel ketulian dan penanganan
kesehatan indera di Desa Bengkala, Buleleng, Bali. Buletin Penelitian Sistem
Kesehatan 15: 1-7.
7.
Patrick DL, Edward TC, Skalicky AH, Schick B, Topolski
TD, et al. (2011) Validation of quality of life measure for deaf or hard of
hearing youth. Otolaryngol Head Neck Surg 145: 137-145.
8.
Borujeni SS, Hatamizadeh N, Vameghi R (2015) Hearing
loss related quality of life in adolescents with hearing loss. Iran Rehabil J
13: 38-43.
9.
Hurlock EB (2011) Psikologi perkembangan suatu
pendekatan sepanjang rentang kehidupan. 5th Edn. Jakarta: Erlangga.
10.
Ebrahimi H, Mohammadi E, Pirzadeh A, Shamshiri M,
Mohammad A (2017) Living with worry: The experience of mothers with deaf child.
Int J Pediatr 5: 42.
11.
Khotimah N (2009) Penerimaan Ibu yang Memiliki Anak
Tunarungu. Available at: http://www.gunadarma.ac.id/library/graduate/psychology
12.
Wasito DS, Sarwindah D, Sulistiani W (2010)
Penyesuaian sosial siswa tuna rungu di sekolah umum. Jurnal Psikologi Teori dan
Terapan 2: 138-152.
13.
Marthan, LK (2007) Manajemen pendidikan inklusif.
Jakarta: Departemen Pendidikan Nasional.
14.
Fellinger J, Halzinger D, Pallard R (2012) Mental
health of deaf people. Lancet 379: 1037-1044.
15.
Alwis C (2005) Children with hearing Impairment in
regular classroom. Sri Lanka J Educ Res 9: 45-69.
16.
Suarbhawa IGM, Sunarya IN (2009) Laporan Penelitian
Arkeologi Survei Epigrafi Kubutambahan Buleleng. Denpasar: Balai Arkeologi
Denpasar.
17.
Donaldson P, Langham E, Best T, Browne M (2015)
Validation of the gambling perceived stigma scale (GPSS) and the gambling
experienced stigma scale (GESS). J Gambling Issues 31: 163-200.
18.
Santrock WJ (2008) Psikologi Pendidikan. Jakarta:
Prenada Media Group.
19.
Batten G, Oakes PM, Alexander T (2013). Factors
associates with social interactions between deaf children and their hearing
peers: A systematic literature review. United Kingdom: Department of Clinical
Psychological Therapies, The University of Hull.
20.
Leary MR (2010) Affiliation, acceptance and belonging:
The pursuit of interpersonal connection. Dalam: Fiske ST, Gilbert DT, Lindzey G
(penyunting). Handbook of social psychology. Hoboken, NJ, US: John Wiley &
Sons Inc., pp: 864-897.
21.
Kurniati DPY, Suariyani NLP, Listyowati R, Mangunsong
F, Pratomo H, et al. (2013) Pemahaman dan penerimaan anggota sekaa teruna
teruni terhadap warga kolok di desa Bengkala, kecamatan Kubutambahan, Buleleng,
Bali. Available at: https://simdos.unud.ac.id/
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- International Journal of Diabetes (ISSN: 2644-3031)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)


