630
Views & Citations10
Likes & Shares
One of the drawbacks in chemotherapy of cancer is to determine cure-effective dosing [1]. In biological system, the dose response curve is generally sigmoidal in shape exhibiting a lag phase, a linear accelerating log phase and reaching an asymptote or a plateau phase finally. It is expected that in the linear log phase, the higher dose limit is expected to give a promising result of the total or nearly total loss of cancer cells. On the contrary, in clinical practice the drugs revealed a reduction in the anti-tumor activity in reality and as a consequence 20% residual tumor cells/cancer cells remain alive and their elimination becomes formidable in oncology. Moreover in clinical settings, all chemotherapeutic drugs of one kind or another would cause inadvertent side effects [2,3]. The reasons for the survival of some cancer cells are manifold.
• In the primary population of cancer cells at the primary lesion site, about 0.8 to 1% cells are stem cells which are both radiation-resistant and chemo resistant.
• Secondly not all cells are cytotoxically killed by the chemo drug, though the cells represent a clonal population, some remain intact and develop cellular resistance by the genetic modulation, similar to particulate antigens. Such resistance could be expected, in view of the drugs applications. Since anticancer drugs are often associated with general toxicity to normal cells, physical side effects and hematological disorders, clinicians often either reduce the dose or increase the time in travel between each cycle of the treatment in order to avoid the acute toxicity [4].
The concept of dose intensity was put-forth by Hryniuk and Goodyear [5] where the dose intensity refers to the amount of the drug per unit of time, i.e., mgms/square-meter/week, irrespective of the route of administration or the schedule [4,5].
Clinical practices have documented evidence for a positive relationship between the dose intensity and response rates in several solid tumors including advanced ovarian, breast, lung and colon cancers as well as in hematologic malignancies such as the lymphomas.
As of now three modes of approaches to deliver chemotherapeutic drugs in a dose intense manner have been in vogue in the clinical setting viz.
• The first approach is by dose escalation whereby the doses of the anti-cancer drugs are increased in quantum.
• The second approach is to administer the anti-cancer agents in a dose dense manner by reducing the interval between treatment cycles.
• The third strategy involves sequential scheduling of either single agent or combination regimens.
• It is of interest to note that, so far these three modus operandi of drug dosing had been practiced irrespective of the immune status of the patient subject.
The cytotoxic killing of cancer cells at the log phase, by the drugs in chemotherapy would be greater in tumors of smaller volume. In the latter case residual cancer cells and their regrowth is not uncommon. In chemotherapy more frequent administration which is considered a simple maneuver has also benefitted the tumor load or burden.
For instance, a study have shown that a dose dense schedule of doxorubicin, cyclophosphamide and Paclitaxel when administered, on an every 2 week schedule instead of conventional 3 week interval significantly improved the clinical outcomes with respect to disease free survival (DFS) and overall survival (OS). Dose dense approach strategy was also reported to be effective in the treatment of metastatic cases, like colorectal, small cell lung and germ cells cancers [6,7].
There exists a controversy whether combination chemotherapy could yield superior response than sequential single agent therapy. Prior investigation have revealed that combination therapy involving two agents, though have yielded a superior response rate it did not improve the patient’s quality of life, and did not translate into a survival benefit. Their investigations also revealed that sequential chemotherapy involving a single agent will be the reasonable treatment option in patients with metastatic breast cancers [8].
The chemotherapeutic domain no doubt has made a sea change in cancer treatment. However we have to go a long way, and we need to find still new treatment approaches. In this context, understanding cancer biology and the cellular kinetics of cancer cells besides to drugs, to other phytonutrients are of interest and research towards their applications to cancer patients will constitute an important paradigm shift.
In chemotherapy, metastatic cancers are still a challenging task. The dissemination of malignant cells to distant organs occurs through blood stream, lymph, and by cells movement to adjacent nodal regions and also to the abdominal cavity. Investigation has opined that the prior identification of the sites of primary cancer cells is tantamount to a prospective cure. But in case of metastasis through hematogenous and lymphatic dissemination and their settlement in distant organs, chemotherapeutic drugs to target these secondary regions or organs is of paramount importance. Towards this end, complete kill in secondary sites/organs in often met with failures [7].
The intersection between metastasing cancer cells (which are recapitulated embryonic cells) and the target organ might involve the immunosuppressive factors through gain of gene signatures so as to remain free from the host’s immunosurveillance.
To tackle the metastasis undertaking cells, research has to be revamped to:
I. Neutralize the proteomic factors of the secondary organs.
II. Delimit the immune-suppressors of both the secondary organ and the cancer cells.
III. Activation/reactivation of silenced immune cells like the dendritic and NK cells.
The above three notions could be realized through phytochemical nutrient adjuvants. Since metastatic cancer cells invade through systemic route (blood) and lymph diverse strategies are needed to reactivate the immune system and its plethora of cytotoxic cells through phytonutrients, or the organic plant molecules. The synergistic-co action of chemical drugs, biomolecules/phytonutrient compounds and a revamped immune system certainty could save millions of dying cancer patients. Thus far, only immunologically strong patients have won the cancer war. The witness of such candidates (case study) is the strong evidence [9].
In our laboratory studies on cell line (SP2/o myeloma cells) we have observed that green tea and black tea extract (both hot and cold), calotropis plant latex and Nerium latex diluted in PBS with 1:100 ratio and their cytotoxic effects. The calotropis latex, have brought 100% cell death or nearly 100% cell death (MTT assay and trypan blue cell viability assay. The employed herbal products are known for monophenols, polyphenols, alkaloids and catechins, etc. Phytonutrients containing various anticancer compounds like flaovonoids, isoflavonoids, carotenoids, catechins, mono and polyphenols, terpenoids, etc., may be representing a strong armamentarium against the cancer cells. As far as the disease cancer is concerned the abnormal diets and life style are considered as causal factors. To antagonize the cancer cells and to ameliorate the cancer disease, oral phytonutrients or nutrient adjuvants are the solution. The beneficial effects of phyto-nutrients in curing cancer remains in their anti-inflammatory, antimicrobial and anti-carcinogenic properties. Even the metastatic stages could be reversed by the dietary adjuvants [10,11].
For instance, the flavonoids present in some food supplements like the grape fruit extract, red wine, grape seeds protect the ascorbic acid (Vit-C) by their specific charge transfer interactions. Moreover flavonoids by chelating the copper ions could inhibit the enzymic and non-enzymic oxidation of ascorbic acid. Of all free radical scavenging effect of flavonoids would prevent the formation of a new generation of malignant cells. In this context the chemotherapeutic drugs cause free radicals formation is of interest, since it may offset the action of phytochemical molecules antioxidants. The next category phytochemical compounds present in the tea and other food plants are the phenols, mono-phenols and poly-phenols. When it is phenol it can combine with D-glucose and Gallic acid and form polyphenols in vivo. Hence the polyphenols in plant foods may act as anti-cancer compounds, that is, they can deprive the availability of glucose to the malignant cells and thus can interfere with their metabolism and growth. Like phenols the tannins are also known to bind with the glycoprotein [12].
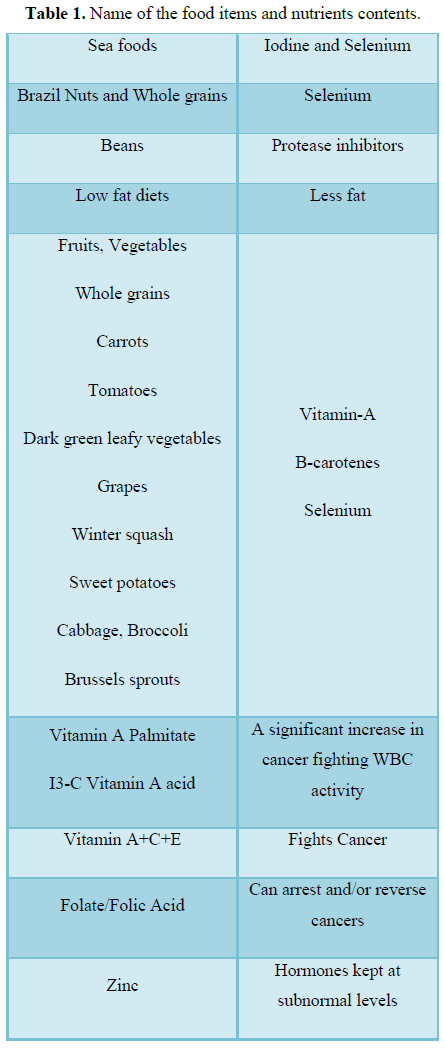
Yet another beneficial effect of phenolic compounds in cancer fighting phytonutrients or nutrient adjuvants is their nitrate scavenging function which helps to inhibit nitrosamine formation and tissue carcinogenesis. Some other phytochemical compounds like isoflavonoids, phytoalexins such as glyceollin, phaseollin and pisatin are cytotoxic in nature and can affect cell death in tumor mass (Table 1).
CONCLUSION
In summary, the therapeutic attacks over metastazing cancer cells ought to be multi-prolonged alongside chemotherapy, to cause manifold changes viz., protease inhibitor phytomolecules inhibiting the glucose supply and the cancer cells glycolytic process; inhibiting the production of lactic acid in cancer cells in their micro environment; enhancing the antioxidants to reduce free radicals load; inhibiting the cox-2 enzyme activity and thereby preventing the conversion of Arachidonic acid into PGE-2, the promoter of cancer cells divisions, through CoX-2 inhibitors like non steroid anti-inflammatory drugs (NSADS) as annexing drugs; and finally immunologically potentiating the cytotoxic cells. In this context the 2018 noble prize winners for medicine Tasuku Honjo and James Allison and their contribution of “negative immune regulation or immune checkpoint therapy” by preventing the blockade protein molecules CTLA-4 and PD-1 and in unleashing the immune cells to attack the cancers cells in patients with advanced cancers is of interests, in immunotherapy which is promising to boost disease free survival (DFS) and overall survival (OS). The phytochemical molecules in curing the cancer by their cytotoxicity is a feasible venture, because these phytochemical compounds are known to inhibit certain pathways which the cancer cells exploit for their proliferation, and at the same time enhance certain genes to act against the cancer cells and promote their apoptosis through caspase-3 pathway. Our personal laboratory observation of the beta-carotene on aneurysm developed in knockout mice revealed that beta-carotene not only ameliorated the above aneurysm the experimental mice, but also revealed a conspicuous wait/size increment in spleen which is an important immunological organ playing important role in cytotoxicity [13-15].
CONFLICT OF INTEREST STATEMENT
The authors have declared that no conflict of interest exists.
1. Tackling RA (2013) The problems of tumor chemotherapy by optimal drug scheduling. J Clin Diagn Res 7: 1404-1407.
2. Li L, Mok H, Jhaveri P, Bonnen MD, Sikora AG, et al. (2018) Anti-cancer therapy and lung injury: Molecular mechanisms. Expert Rev Anticancer Ther 18: 1041-1057.
3. Belenkov YN, Privalova EV, Kozhevnikova MV, Kirichenko YY (2018) Vascular complications of cancer chemotherapy. Kardiologiia S9: 4-9.
4. Hryniuk WM (1987) Average relative dose intensity and the impact on design of clinical trials. Semin Oncol 14: 65-74.
5. Hryniuk WM, Goodyear M (1990) The calculation of received dose intensity. J Clin Oncol 8: 1935-1937.
6. Gluck S (2005) Adjuvant chemotherapy for early breast cancer: Optimal use of epirubicin. Oncologist 10: 780-791.
7. Ladwa R, Kalas T, Pathmanathan S, Woodward N, Wyld D, et al. (2018) Maintaining dose intensity of adjuvant chemotherapy in older patients with breast cancer. Clin Breast Cancer 18: e1181-e1187.
8. Sledge GW, Neuberg D, Bernardo P, Ingle JN, Martino S, et al. (2003) Phase III trial of doxorubicin, paclitaxel and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: An intergroup trial (E1193). J Clin Oncol 21: 588-592.
9. McCarty MF (2001) Current prospects for controlling cancer growth with non-cytotoxic agents - Nutrients, phytochemicals, herbal extracts and available drugs. Med Hypotheses 56: 137-154.
10. Wilson HK, Price-Jones C, Hughes RE (1976) The influence of an extract of orange peel on the growth and ascorbic acid metabolism of young guinea pigs. J Sci Food Agric 27: 661-666.
11. Satgg JV, Milln D (1975) The nutritional and therapeutic value of tea - A review. J Sci Fd Agri 26: 1439-1459.
12. Athanasiadou S, Githiori J, Kyriazakis I (2007) Medicinal plants for helminth parasite control: Facts and fiction. Animal 1: 1392-1400.
13. Gopal K, Gowtham M, Sachin Singh Mani MR, Kamarul Shankar EM (2015) Attrition of hepatic damage inflicted by angiotensin II with α-tocopherol and β-carotene in experimental apolipoprotein E knock-out mice. Sci Rep.
14. Gopal K, Nagarajan P, Shankar EM, Kumar JM, Kamarul T (2014) Angiotensin II-induced aneurysm concurrently elicits splenic hypertrophy and β-carotene ameliorates splenic pathology in Apoe-/- mice. Eur J Clin Investig.
15. Gopal K, Nagarajan P, Jedy J, Raja AT, Gnanaselvi KV, et al. (2013) β-carotene attenuates angiotensin II-induced aortic aneurysm by alleviating macrophage recruitment in Apoe-/- mice. PLoS One.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Alcoholism Clinical Research
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Spine Diseases
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- International Journal of AIDS (ISSN: 2644-3023)


