906
Views & Citations10
Likes & Shares
Basal cell carcinoma (BCC) is the most common
form of cancer, affecting approximately 2 million people in the United States
annually. Abnormal activation of hedgehog signaling plays an important role in
BCC. Two inhibitors of the Smoothened (SMO) component of the hedgehog pathway,
vismodegib and sonidegib, are currently approved for use in advanced BCC
(locally advanced BCC and metastatic BCC), depending on the country of
approval. Location of lesions and fears about changes in appearance may affect
the quality of life (QoL) of patients with advanced BCC. The key clinical
trials for vismodegib (ERIVANCE and STEVIE) and for sonidegib (BOLT) included
QoL as secondary end points. In ERIVANCE, the Short Form-36 showed no changes
from baseline on either the physical or emotional domains. In STEVIE, the
Skindex-16 showed that treatment with vismodegib was associated with clinically
meaningful improvement in the emotional domain. BOLT used predetermined
subscales relevant to advanced skin cancer specifically from the European
Organisation for Research and Treatment of Cancer (EORTC) QLQ-C30 and the EORTC
H&N35. Both the QLQ-C30 and H&N35 selected subscales showed either
maintenance or improvement from baseline. Factors that affect QoL during
treatment of patients with advanced BCC include baseline QoL, having fewer
comorbidities, and having better initial mental health status. In addition,
patients whose lesions were advanced, but were not as large as others or not
located in visible areas (ie, head and neck) reported better QoL.
Treatment-emergent adverse events (AEs) have an impact on QoL in patients with
advanced BCC. Most of the AEs reported in trials for vismodegib and sonidegib
were grade 1–2. Using techniques to manage AEs effectively may help improve QoL
for those whose QoL decreases during treatment.
Keywords: basal cell carcinoma; hedgehog inhibitor;
quality of life; sonidegib; vismodegib
Abbreviations: AE: Adverse Event; BCC: Basal Cell Carcinoma; BCCNS: BCC-Nevus Syndrome; BL: Baseline; CES-D: Center for Epidemiological Studies Depression Scale; EORTC: European Organisation for Research and Treatment of Cancer; EORTC QLQ-C30: EORTC Quality of Life Questionnaire; EORTC H&N35: EORTC Quality of Life Module for Head and Neck Cancer; laBCC: Locally Advanced BCC; mBCC, metastatic BCC; MCS: Mental Component Score; mDOR: Median Duration of Response; PCS: Physical Component Score; PTCH1: Patched1; ORR: Objective Response Rate; QoL: Quality of Life; RECIST: Response Evaluation Criteria in Solid Tumors; SCC: Squamous Cell Carcinoma; SF-36: Short Form-36; SMO: Smoothened
INTRODUCTION
Nonmelanoma skin cancers—basal cell carcinoma (BCC) and squamous cell
carcinoma (SCC)—are the most common malignancies affecting light-skinned
individuals worldwide, and the incidence is increasing. The highest rates of
BCC are seen in Australia (>1000/100,000 person-years) [1]. BCC and SCC are
associated with exposure to ultraviolet radiation from sunlight, and therefore
most often occur on visible parts of the body, such as the head and neck.
Abnormal
activation of the hedgehog signaling pathway plays an important role in BCC development.
Dysregulated signaling by mutated components of hedgehog signaling, especially
Patched1 (PTCH1) and Smoothened (SMO), lead to continual activation of this
pathway [2,3]. Such constant signaling activity affects cellular proliferation,
invasion, and survival, especially in BCC. Therefore, two inhibitors of the SMO
component of hedgehog signaling, vismodegib and sonidegib, were developed and
approved for use in advanced forms of BCC (locally advanced BCC [laBCC] and
metastatic BCC [mBCC]), depending on the country of approval (sonidegib is
approved for advanced BCC in Australia and Switzerland and for locally advanced
BCC in the European Union and the United States) [2,3].
Since surgery is frequently used to treat BCC, cosmetic concerns may
occur as a result of treatment, and these considerations may negatively affect
the quality of life (QoL) of patients with BCC [4-6]. Patients with BCC-nevus
syndrome (BCCNS) have multiple BCC lesions, odontogenic keratocysts, palmar or
plantar pits, and other abnormalities. Patients with BCCNS had decreased overall
QoL, as observed in a study of 32 patients who completed the Skindex-29 QoL
survey and the Center for Epidemiological Studies Depression Scale (CES-D).
Moreover, the study results showed that depressive symptoms were particularly
prevalent, with 50% of patients with BCNS having significant depressive
symptomatology [7].
Predictors of how treatment for BCC may affect QoL have been examined.
In one study of 633 patients with BCC or SCC, the single biggest QoL predictor
post-treatment was the skin-related QoL prior to treatment versus
post-treatment: for skin-related QoL, a 20-point difference between the prior
to and after treatment score would indicate that clinically meaningful
improvement in QoL had occurred as a result of treatment [8]. In a second study
of 633 patients with BCC or SCC, QoL outcomes were similar after two common
treatment modalities, Mohs surgery and excision [9]. Fewer comorbidities and
better mental health status were independent predictors as well; however, tumor
characteristics (histological type, location on head or neck, tumor diameter,
noted histological risk factors for recurrence) were not predictors of QoL
[10]. Moreover, patients with minimal clinical involvement may still be highly
distressed, highlighting the patient-dependent variation in QoL associated with
BCC and its treatment [10]. The goal of this brief review is to discuss the
current literature on QoL regarding hedgehog inhibitors for advanced forms of
BCC, with emphasis on trial data.
Assessing QoL in the
ERIVANCE, STEVIE, and BOLT Trials
Vismodegib and sonidegib were approved based on results from
randomized, multicenter trials, ERIVANCE (NCT00833417), STEVIE (NCT01367665),
and BOLT (NCT01327053) [11-13]. All three trials included QoL as secondary end points
but differed in the questionnaires used. In ERIVANCE, QoL was assessed (at
baseline, week 12, week 24, and end of study) by changes from baseline on the
Short Form (SF)-36 questionnaire, which recorded responses to 36 questions
across 8 domains [14]. In STEVIE, the Skindex-16 questionnaire was used to
assess how often patients were troubled by different aspects of their disease
[10]. In BOLT, QoL was measured (at baseline, and every 12 weeks throughout the
study) using relevant predetermined subscales of the EORTC QLQ-C30 (European
Organisation for Research and Treatment of Cancer Quality of Life
Questionnaire) and the EORTC H&N35 (EORTC Quality of Life Module for Head
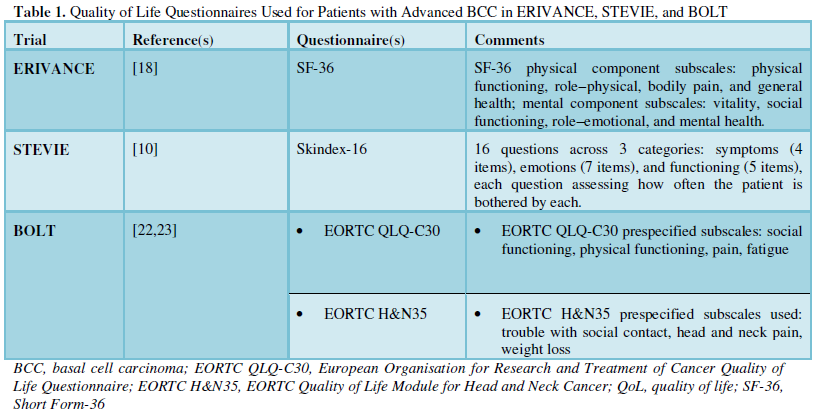
and Neck Cancer) [15,16]. The QoL instruments used in ERIVANCE, STEVIE, and
BOLT differed in their assessments of the impact treatment would have on
patients with BCC (Table 1). Only
BOLT used questionnaires specific for patients with cancer.
QoL from the
ERIVANCE Trial
ERIVANCE, the pivotal study on which approval for vismodegib was based
in the United States, was a phase 2, multicenter, randomized trial. End points
in ERIVANCE were evaluated by investigators and also by an independent, central
review committee (first 12 months solely). Patients in ERIVANCE were evaluated
using Response Evaluation Criteria in Solid Tumors (RECIST) criteria, as assessed
by computed tomography or magnetic resonance imaging [17]. This single-arm,
2-cohort study had 104 patients with advanced BCC enrolled. Of these, 71 had
laBCC and the remainder had mBCC. The objective response rates (ORR; primary
end point) were 43% for patients with laBCC and 30% for patients with mBCC. By
central review, the median duration of response (mDOR) was 7.6 months (range,
1.0–12.9) for patients with laBCC and 7.6 months (range, 2.1–11.1) for patients
with mBCC [17]. Treatment-associated adverse events (AEs) included muscle
spasms, alopecia, and dysgeusia. Most AEs were grade 1-2 [17].
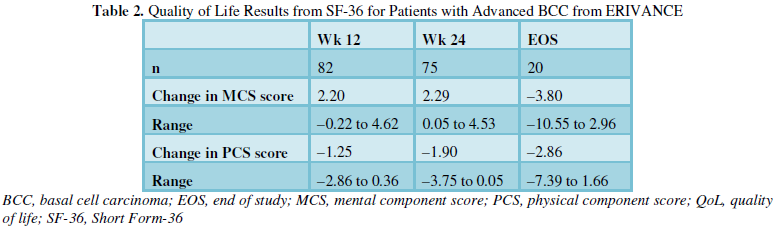
ERIVANCE measured changes in QoL at baseline, weeks 12 and 24, and end
of study or termination. Changes in QoL were assessed by changes from baseline
on the Short Form (SF)-36 questionnaire, as one of its secondary end points
[18]. This single-page questionnaire poses 36 questions across 8 domains:
physical functioning, role limitations due to physical health, role limitations
due to emotional problems, energy or fatigue, emotional well-being, social
functioning, pain, and general health (Table
1). A higher positive score on the SF-36 indicated better QoL [14]. The
SF-36 was not designed to assess the QoL associated with skin disease but is a
general assessment of QoL. At the end of the ERIVANCE study, patients
maintained QoL as shown by the physical and emotional portions of the SF-36 (Table 2) [18].
QoL from the STEVIE Trial
STEVIE was an open-label, multicenter, postapproval trial for
vismodegib having the largest enrollment of patients with advanced BCC at the
time: 499 patients with laBCC and 31 with mBCC. End points in STEVIE were
evaluated by investigators only, and not by a central review committee [19]. After 12 months, the primary end point
was evaluated (percentage of participants who experienced any AEs, grade 3 or 4
AEs, AEs leading to drug interruptions or discontinuations, or any serious AEs)
[12]. Regarding efficacy, STEVIE showed that 302 patients with laBCC had a
response, of whom 153 had a complete response. Of 31 patients with mBCC, 11 had
a complete response. Treatment-emergent AEs were frequent, occurring in 98% of
patients who had <12 months exposure and in 99% of patients who had ≥12
months exposure. The most common of the latter were muscle spasms, alopecia,
dysgeusia, and weight loss [12].
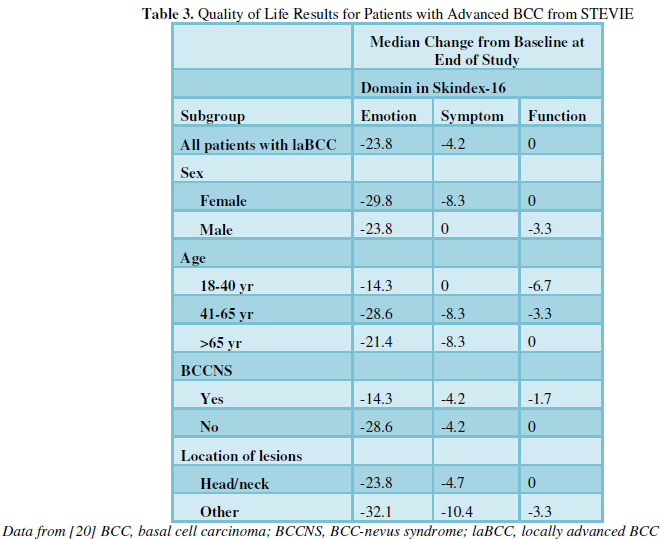
Results
from the Skindex-16 questionnaire from STEVIE (Table 3) showed that patients given vismodegib had clinically
meaningful improvement in the emotional domain [12,20,21]. There were slight
improvements noted in the functional and symptom domains, of which only the
improvement in the emotion scores were consistent with clinical responses (Table 3) [20].
QoL from the BOLT Trial
BOLT
differed from ERIVANCE and STEVIE in evaluating response to treatment in that
investigator as well as central review assessments were used throughout the
42-month trial duration. More stringent RECIST (BCC-modified RECIST;
BCC-mRECIST) criteria were used to evaluate patients in BOLT than were used in
ERIVANCE or STEVIE [22]. BCC-mRECIST is a multimodal tumor assessment method
integrating magnetic resonance imaging per RECIST v1.1, standard and annotated
color photography per World Health Organization guidelines, and histology in
multiple biopsy specimens surveying the lesion area. Partial responses required
a ≥30% decrease in the sum of the longest diameters of target lesion(s) per
RECIST v1.1 (imaging assessments) and a ≥50% reduction in the sum of the
products of perpendicular diameters of target lesion(s) per WHO guidelines.
Complete responses required total resolution of all lesions confirmed on
repeated assessments ≥4 weeks apart by all modalities, and negative
histological results [22]. Had less stringent response criteria been used in
BOLT, the complete response rates would have been similar to those reported in
ERIVANCE [13]. In BOLT, 230 patients were treated after randomization to two
doses of sonidegib, 200 mg or 800 mg given once per day. At 30 months in
patients with laBCC, the ORRs in the 200-mg arm were 56.1% (central review) and
71.2% (investigator review); in the 800-mg arm, ORRs were 45.3% and 58.6%,
respectively. By central review, mDOR was 26.1 months for patients with laBCC
and 24.0 months for patients with mBCC [13]. These were longer than the mDOR
seen for vismodegib in ERIVANCE (7.6 months for both laBCC and mBCC) [17].
Data from the 30-month analysis of BOLT in patients with mBCC showed
ORRs in the 200-mg arm were 7.7% (central review) and 23.1% (investigator
review); in the 800-mg arm, the ORRs were 17.4% (central review) and 34.8%
(investigator review), respectively [13]. The most frequent AEs leading to
treatment discontinuation were muscle spasm (3 [4%] in the 200-mg group vs. 13
[9%] in the 800-mg group), dysgeusia (2 [3%] vs. 7 [5%]), weight decrease (2
[3%] vs. 7 [5%]), and nausea (2 [3%] vs. 6 [4%]) [13].
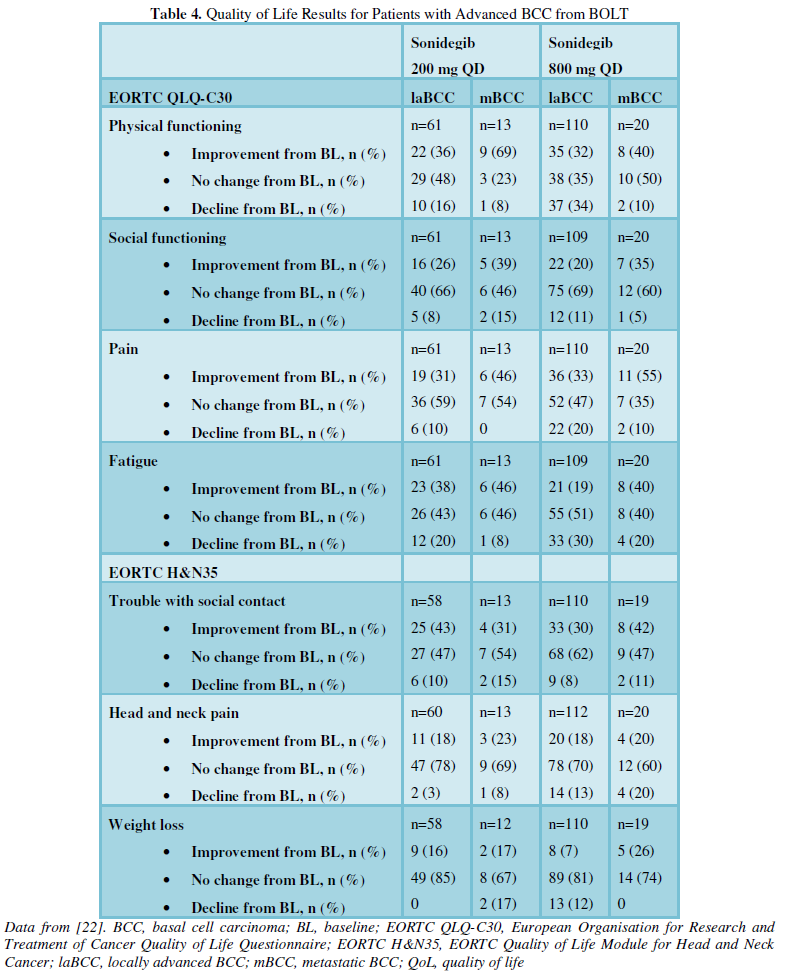
QoL in
BOLT was monitored at baseline, every 12 weeks, and at the 18-month
prespecified end point. At 12 months, 82% of patients were still responding to
sonidegib, the median duration of response had not yet been reached, and the
majority of patients had maintenance of or improvement in predetermined
subscale scores on the EORTC QLQ-C30 and the EORTC H&N35. Improvements in
QLQ-C30 and H&N35 were found to be consistent across laBCC and mBCC cohorts
(Table 4). This analysis showed
>80% of patients reported maintenance or improvement in each predetermined
subscale through week 73 (Table 4)
[22-24]. The results of the EORTC H&N35 showed the most improvement in the
domain of trouble with social contact, an indication that sonidegib may have
improved some patients’ concerns regarding the effect of advanced BCC on their
appearance (Table 4).
RECIST vs BCC-mRECIST
Patients with laBCC in ERIVANCE were evaluated using a composite end
point: a decrease of ≥30% in the externally visible or radiographic dimension
or complete resolution of ulceration, if present at baseline [17].
In BOLT, more stringent RECIST criteria were used to evaluate patients
with laBCC. BCC-modified RECIST (BCC-mRECIST) is a multimodal tumor assessment
method integrating magnetic resonance imaging (MRI) per RECIST v1.1, standard
and annotated color photography per World Health Organization guidelines, and
histology in multiple biopsy specimens surveying the lesion area. Partial
response in lesions assessed by MRI required a ≥30% decrease in the sum of the
longest diameters of target lesion(s) per RECIST v1.1 (imaging assessments) and
in lesions assessed by photography, a ≥50% reduction in the sum of the products
of perpendicular diameters of target lesion(s) per WHO guidelines. Complete
responses required total resolution of all lesions confirmed on repeated
assessments ≥4 weeks apart by all modalities, and all of multiple biopsies
yielding negative histological results [22].
DISCUSSION
BCC affects QoL variably, depending upon stage of disease and symptoms.
In a recent study of 34 patients with BCC (21 of whom had advanced BCC), 95% of
patients with advanced BCC identified their symptoms as bothersome, compared
with 69% of patients with BCC. Over three-quarters (76%) of patients with
advanced BCC reported limiting their daily activities as a result of their
disease, compared with 46% of patients with BCC. Furthermore, 57% of patients
with advanced BCC reported limiting activities (eg, exposure to sun, or
strenuous activities in part due to surgery), compared with 31% of patients
with BCC [25].
Patients with BCCNS reported decreased QoL, and for these patients,
depressive symptoms were more prevalent [7]. The impact of treatment for BCCNS
was evaluated using the Skindex-29 in this study [7]. Patients with BCCNS are
often treated with surgery; this study evaluated the extent to which multiple
surgeries affected QoL. Investigators found that patients treated with surgery
scored significantly lower on the CES-D scale for depressive symptoms than did
patients not treated with surgery (lower scores on the CES-D scale indicate
fewer depressive symptoms) [7]. In a second study, patients with BCCNS were
compared with patients with advanced BCC. The investigators observed that
patients with BCCNS had profiles similar to those of patients with chronic
illness, whereas the profile of patients with advanced BCC resembled more
closely patients with acute illnesses [26].
Nonsurgical, nonpharmaceutical treatment of BCC (radiation therapy) was
shown to affect the QoL of patients with BCC. One study compared patients with
BCC treated with X-ray therapy with healthy, matched individuals (25 in each
cohort). The patients’ Dermatology QoL Index decreased significantly,
indicating improvement in scores, at 3 months following treatment and were
similar to the scores of matched healthy control subjects. The subcategory most
affected was Symptoms and Feelings, which showed a significant decline in score
from baseline to 3 months after treatment [27]. It is interesting to note that
the Daily Activities subcategory showed no significant change from baseline
following therapy.
Finally, the impact of treatment-emergent AEs on QoL should be
discussed. Unlike targeted therapies approved for other types of cancer (eg,
sorafenib, imatinib), which can cause various cutaneous AEs (among them
hypopigmentation, maculopapular rash, and epidermoid cysts) [28,29], alopecia
is the main cutaneous AE resulting from treatment with hedgehog inhibitors [28].
Common noncutaneous AEs include muscle spasm, dysgeusia, fatigue, and nausea
[11,22]. Moreover, although the majority of the AEs reported for vismodegib and
sonidegib were grade 1-2, it should be noted that patients may take either of
these drugs for a longer term [30,31], so managing AEs may lead to higher QoL
and increased treatment effect, due to more consistent drug exposure. For
example, diarrhea may be treated with loperamide 2 mg up to 16 mg daily, and
alopecia may respond to 5% topical minoxidil twice daily [32].
CONCLUSIONS AND
SUMMARY
The approval of two hedgehog inhibitors for laBCC and mBCC, vismodegib
and sonidegib, changed the treatment paradigm for patients with advanced forms
of BCC. The approvals were based on results from the ERIVANCE and STEVIE trials
for vismodegib and the BOLT trial for sonidegib. Because advanced BCC most
often occurs on the more visible parts of the body such as the head and neck,
patients may be concerned about appearance, and these worries may adversely
affect their QoL. Changes in QoL from baseline in the ERIVANCE, STEVIE, and
BOLT trials ranged from no change to improvements in several domains
[11,19,22]. Although the AE profiles of approved hedgehog inhibitors have fewer
high-grade events compared with other targeted therapies, the impact of
commonly occurring AEs on QoL should not be discounted due to their chronic and
bothersome aspects, which may limit use of these therapies. More effective AE
management should help improve QoL for patients with advanced BCC who are at
risk of experiencing decreased QoL during their course of treatment.
ACKNOWLEDGMENT
Medical
writing support was provided by Beverly E. Barton, PhD, ScioScientific, LLC.
FINANCIAL SUPPORT
Publication of this review was supported by Sun Pharmaceutical Industries, Ltd. The author received no compensation for writing it. Dr. Migden has participated on advisory boards with and received honoraria from Genentech, Inc., Novartis Pharmaceuticals Corporation, Sun Pharmaceutical Industries, Ltd., and Eli Lilly & Company.
1. Lomas
A, Leonardi-Bee J, Bath-Hextall F (2012) A systematic review of worldwide
incidence of nonmelanoma skin cancer. Br J Dermatol 166: 1069-1080.
2. Peukert
S, Miller-Moslin K (2010) Small-molecule inhibitors of the hedgehog signaling
pathway as cancer therapeutics. Chem Med Chem 5: 500-512.
3. Zheng
X, et al. (2013) Role of the hedgehog pathway in hepatocellular carcinoma
(review). Oncol Rep 30: 2020-2026.
4. Philipp-Dormston
WG, et al. (2017) Patient-reported health outcomes in patients with
non-melanoma skin cancer and actinic keratosis: results from a large-scale
observational study analysing effects of diagnoses and disease progression. J
Eur Academy Dermatol Venereol. [in press]
5. Gaulin
C, Sebaratnam DF, Fernández-Peñas P (2015) Quality of life in non-melanoma skin
cancer. Aus J Dermatol 56: 70-76.
6. Lanoue
J, Goldenberg G (2016) Basal cell carcinoma: a comprehensive review of existing
and emerging nonsurgical therapies. J Clin Aesthetic Dermatol 9: 26-36.
7. Shah
M, et al. (2011) Quality of life and depression assessment in nevoid basal cell
carcinoma syndrome. Int J Dermatol 50: 268-276.
8. Chen
T, et al. (2007) Predictors of skin-related quality of life after treatment of
cutaneous basal cell carcinoma and squamous cell carcinoma. Archives Dermatol
143: 1386-1392.
9. Chren
MM, et al. (2007) Quality-of-life outcomes of treatments for cutaneous basal
cell carcinoma and squamous cell carcinoma. J Investigative Dermatol 127:
1351-1357.
10.
Chren MM (2012) The Skindex instruments to measure the effects of skin disease
on quality of life. Dermatologic Clinics 30: 231-236.
11.
Sekulic A, et al. (2017) Long-term safety and efficacy of vismodegib in
patients with advanced basal cell carcinoma: final update of the pivotal ERIVANCE
BCC study. BMC Cancer 17: 332.
12. Basset-Seguin
N, et al. (2015) Vismodegib in patients with advanced basal cell carcinoma
(STEVIE): a pre-planned interim analysis of an international, open-label trial.
Lancet Oncol 16: 729-736.
13. Lear
JT, et al. (2018) Long-term efficacy and safety of sonidegib in patients with
locally advanced and metastatic basal cell carcinoma: 30-month analysis of the
randomized phase 2 BOLT Study. J Eur Acad Dermatol Venereol. 32: 372-381.
14. Ware
JE, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36).
Medical Care 30: 473-483.
15. Aaronson
NK, et al. (1993) The European Organization for Research and Treatment of
Cancer QLQ-C30: a quality-of-life instrument for use in international clinical
trials in oncology. J Natl Cancer Inst 85: 365-376.
16. Bjordal
K, et al. (1999) Quality of life in head and neck cancer patients: validation
of the European Organization for Research and Treatment of Cancer Quality of
Life Questionnaire-H&N35. J Clin Oncol 17: 1008-1019.
17. Sekulic
A, et al. (2017) Long-term efficacy and safety of vismodegib in patients with
advanced basal-cell carcinoma: final update of the pivotal ERIVANCE BCC Study. BMC
Cancer 17: 332.
18. National
Cancer Institute (2017) A study evaluating the efficacy and safety of
vismodegib (GDC-0449, hedgehog pathway inhibitor) in patients with advanced
basal cell carcinoma. Available from: https://clinicaltrials.gov/ct2/show/NCT00833417?term=NCT00833417&rank=1.
19. Basset-Seguin
N, et al. (2017) Vismodegib in patients with advanced basal cell carcinoma:
primary analysis of STEVIE, an international, open-label trial. Eur J Cancer
86: 334-348.
20. Hansson
J, et al. (2015) 3342 Assessment of quality of life using Skindex-16 in
patients with advanced basal cell carcinoma (BCC) treated with vismodegib in
the STEVIE study. Eur J Cancer 51: S680-S681.
21. Grob
JJ, et al. (2016) Assessment of quality of life (QoL) using Skindex-16 in
patients (pts) with locally advanced basal cell carcinoma (laBCC) treated with
vismodegib (VISMO) in the STEVIE study. J Am Academy Dermatol 74: AB193.
22. Migden
MR, et al. (2015) Treatment with two different doses of sonidegib in patients
with locally advanced or metastatic basal cell carcinoma (BOLT): a multicentre,
randomised, double-blind phase 2 trial. Lancet Oncol 16: 716-728.
23. Dummer
R, et al. (2014) Patient-reported quality of life (QOL) with sonidegib (LDE225)
in advanced basal cell carcinoma (BCC). Annals Oncol 25: iv390-iv390.
24. Guminski
A, et al. (2014) Quality of life (QOL) in patients (pts) with advanced basal
cell carcinoma (BCC) treated with sonidegib (LDE225). Pigment Cell Melanoma Res
27: 1195.
25. Steenrod
AW, et al. (2015) A qualitative comparison of symptoms and impact of varying
stages of basal cell carcinoma. Dermatol Therapy 5: 183-199.
26. Mathias
SD, et al. (2014) Assessing health-related quality of life for advanced basal
cell carcinoma and basal cell carcinoma nevus syndrome: development of the
first disease-specific patient-reported outcome questionnaires. JAMA Dermatol
150: 169-176.
27. Skiveren
J, et al. (2012) Skin reactions and quality of life after x-ray therapy of
basal cell carcinoma. J Skin Cancer. 2012: 825095.
28. Tang
N, Ratner D (2016) Managing cutaneous side effects from targeted molecular
inhibitors for melanoma and nonmelanoma skin cancer. Dermatologic Surgery 42:
S40-S48.
29. Tischer
B, et al. (2017) Dermatologic events from EGFR inhibitors: the issue of the
missing patient voice. Supportive Care Cancer 25: 651-660.
30. Genentech
USA (2017) Erivedge prescribing information. South San Francisco, CA.
31. Sun
Pharmaceuticals Industries, Ltd. (2017) Odomzo prescribing information.
Cranbury, NJ.
32. Lacouture
ME, et al. (2016) Characterization and management of hedgehog pathway
inhibitor-related adverse events in patients with advanced basal cell
carcinoma. The Oncologist 21: 1218-1229.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Spine Diseases
- Journal of Alcoholism Clinical Research
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)


