800
Views & Citations10
Likes & Shares
Therapeutic interventions in acute respiratory
distress syndrome (ARDS) primarily depend on lung-protective strategies, as no
disease-modifying treatment has become available. In recent years, mesenchymal
stem cells (MSCs) have been emerged as a new therapeutic option for ARDS, while
among the early phase clinical trials, several studies showed tolerability and
safety rather than efficacy of the MSCs. Here we summarized the results of
published clinical studies on MSCs treatment in ARDS and discussed some approaches
in improving the clinical trial design, aiming to help to enhance the
implementation of cell-based therapy on ARDS.
Keywords:
Stem cells, Acute lung injury, Therapy, Clinical research, Review
Acute respiratory distress syndrome (ARDS) is a severe clinical
condition which may be triggered by various pathologies such as
trauma, pneumonia and sepsis, and characterized by
excessive inflammation in the lungs [1]. Despite fifty years of
research, therapeutic interventions in ARDS remain
primarily limited to supportive strategies, as no disease-modifying treatment
has yet become available [2].
Mesenchymal stem cells (MSCs)
are multipotent stromal cells that
can differentiate into a variety of cell types [3]. Based on
favorable results in preclinical models, MSCs can modulate
the immune response and enhance recovery from lung injury, thus MSCs have
been emerged as a new therapeutic option for ARDS [4]. Encouragingly, case
reports suggested promising therapeutic potential [5,6]. While
among the early phase clinical trials, several studies showed high tolerability
than efficacy of the cells. Here we reviewed the results and designs of published clinical trials of
MSCs in ARDS, trying to explore optimal clinical trial
designs, aiming to help to collect more compelling evidence in new
interventions.
RESULTS OF THE
PUBLISHED CLINICAL TRIALS
Safety
Since the first clinical application of MSCs in 1995, MSCs have
appeared to be well-tolerated with no cell infusion-related evidence of severe
adverse effects (SAEs) in trials of various conditions [7,8]. Similar results
on safety were seen in ARDS clinical trials.
The first clinical case of human umbilical cord MSCs
(HUC-MSCs) therapy in ARDS was documented in 2012 [9].
Five patients with ARDS caused by acute paraquat poisoning received
conventional treatment plus HUC-MSCs at a dose of 1![]() 106 cells/kg body weight (BW) by
I.V. once a day for five consecutive days. No adverse reactions were presented
in the HUC-MSC group, and almost all the major organs function showed normal in
re-examination, except for one case of incompletely absorbed shadow in the lung
from CT scan.
106 cells/kg body weight (BW) by
I.V. once a day for five consecutive days. No adverse reactions were presented
in the HUC-MSC group, and almost all the major organs function showed normal in
re-examination, except for one case of incompletely absorbed shadow in the lung
from CT scan.
In the first completed clinical trial published in 2014using adipose tissue-derived MSCs (AT-MSCs)
to treat ARDS [10], patients with ARDS randomly received one intravenous dose
of 1![]() 106 allogeneic AT-MSCs/kg BW in
100ml normal saline or 100ml normal saline as control. One patient from each
group developed diarrhea and resolved within 48 hours. One patient in MSCs
group presented with rash and resolved spontaneously. One patient in MSCs group
died of multiple organ failures while two patients in placebo group
respectively died of multiple organ failure or sepsis. The deaths were
considered to be related to the preexisting disease processes but not the MSCs
used in the study.
106 allogeneic AT-MSCs/kg BW in
100ml normal saline or 100ml normal saline as control. One patient from each
group developed diarrhea and resolved within 48 hours. One patient in MSCs
group presented with rash and resolved spontaneously. One patient in MSCs group
died of multiple organ failures while two patients in placebo group
respectively died of multiple organ failure or sepsis. The deaths were
considered to be related to the preexisting disease processes but not the MSCs
used in the study.
Bone marrow-derived MSCs (BM-MSCs) are the most
commonly used stem cell types. In a dose-escalation
clinical trial published in 2015 [11], JG Wilson et al. demonstrated that a
single dose of allogeneic BM-MSCs by I.V. infusion was well tolerated in
patients with moderate to severe ARDS. There was no
pre-specified infusion associated events. SAEs were observed in three patients:
two patients expired more than seven days after the MSC infusion, and one
patient got multiple embolic infarcts that thought to have occurred prior the
MSC infusion based on MRI results. None of these SAEs were thought to be
related to MSC infusion.
Efficacy
From the studies above, the treatment of ARDS by MSCs showed good
safety suggesting the possibility of MSCs clinical application, but the
effectiveness evaluation results were divergent.
During the HUC-MSCs therapy study in ARDS caused by acute paraquat
poisoning, the HUC-MSCs group showed significantly lower maximum SOFA scores
and lung injury scores (LISs) than the control group after treatment [9]. More
encouragingly, all the five patients in the HUC-MSCs group
survived, while in the control group, there was only one patient out of eight
survived.
In Zheng G, et al. study, AT-MSCs treatment significantly improved the
patients’ PaO2/FiO2 ratio from baseline and decreased serum SP-D levels at day
5 than those at day 0, suggesting that the MSCs may be effective in reducing
epithelial cell injury, while the PaO2/FiO2, the assessment of hospital indices
and other serum biomarkers did not reveal significant differences between MSCs
and placebo groups [10].
JG Wilson et al. demonstrated changes in LIS and SOFA score with the
high dose of BM-MSCs (10 million cells/kg BW) compared to lower doses [11].
However, this difference was not statistically significant between groups.
Median levels of IL-6, RAGE, and Ang-2 levels all decreased between baseline
and day three, while these markers are known to decline over time in patients
with ARDS treated with low tidal volumes. Thus, without a matched control
group, we cannot conclude that the observed biomarker changes were related to
MSC therapy.
Issues on the
clinical trial design
It is critically necessary to observe clear and significant clinical
benefit in early clinical trials since the increased heterogeneity of
populations and diseases in phase III-IV trials will often weaken the
significance of minor benefits in early trials [12]. But the complex
biological activities of stem cells and various mechanisms of ARDS pathogenesis
have brought difficulties in clinical trials. Various biases caused by in
appropriate design, over-widened or unduly narrowed inclusion/exclusion criteria, improper
interventions, as well as inadequate observation endpoints pre supposed or
results interpretation; each will further impede our seeking for the scientific
truth. Here we listed a selection of problems and challenges in clinical trial
designs on MSCs therapy in ARDS, hoping to contribute to optimized research
projects.
CLINICAL PROTOCOLS
Randomized controlled trials (RCTs) are recognized to provide more
explicit proof of impact since RCTs are possible to avoid all kinds of bias and
balance confounding factors, in which randomization, control, and blinding are
considered as the essential principles [13].
Randomization, a core principle in the RCT, can reduce confounding by
equalizing independent variables that have not been accounted for in the
experimental design [14]. In the published clinical trials above, two of them
didn’t use random allocation procedure [9,11], and the only experiment using
randomization didn’t describe the exact randomly allocating method, so that the
statistical power would be limited and the judgment of the results may be
affected.
Control can determine how much benefit of the subjects regarding safety
and efficacy come from experimental agents. In the dose-escalation clinical
trial, the mortality rate was compared with the
published general mortality rate, and the clinical outcomes and plasma
biomarker levels were compared between different dose groups or using
self-control [11]. Because of the variation in mortality rates and therapeutic
efficiency among hospitals at different times, a placebo control or standard
therapy control is highly recommended.
Blinding can effectively avoid the biases caused by subjective factors
in evaluations. In Liu, W.W.’s study with all the five patients surviving in
the HUC-MSCs and only one out of eight patients surviving in the control group,
either of the researchers or patients were blinded [9]. Therefore, the
reliability of the excellent curative effect might be reduced to a certain degree.
Enrollment criteria
Efficacy trials with well-defined and homogeneous populations are more
probable to produce a clinically meaningful and statistically significant
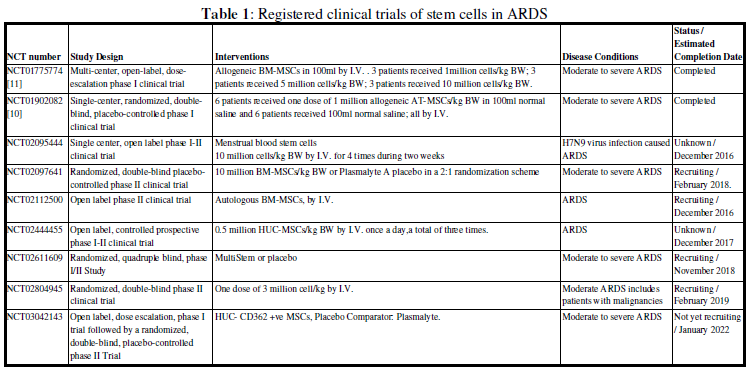
effect [15]. Among the registered nine clinical trials on stem cells in ARDS,
seven studies enrolled all-cause ARDS patients (Table 1). Since ARDS is a heterogeneous clinical syndrome which can
result from multiple conditions, it is likely that the underlying
pathophysiology may be entirely different [16]. This may be one of the reasons why
some clinical trials failed to show improvement in overall survival or various
physiological parameters. Besides, Calfee et al. have identified a
hyper-inflammatory phenotype of ARDS with higher mortality using clinical and
biologic data [17]. When applied to patients in earlier trials, these patients
might be more likely to benefit from MSCs therapy.
INTERVENTIONS
Cell origin, dosage, delivery
route, and cell quality control, are all critical to the therapeutic effect.
Stem cells from different sources have
various characteristics. AT-MSCs showed more potent immunomodulatory effects and greater
proliferation capacity over than BM-MSCs [18], while
umbilical cord blood-derived MSCs showed higher proliferation capacity than
BM-MSCs and AT-MSCs [19]. And there are other optional stem cells
--the endogenous lung stem cells seem to can integrate better into injured lung
tissue [20], and endothelial progenitor cells appear to have therapeutic
effects via differentiation into the endothelium of the damaged vascular site
[21]. Which cell type or mixed multi-stem cells are more suitable for ARDS
treatment remain to be determined by evidence from more preclinical and
clinical research.
In the use of MSCs for ARDS treatment, whether there is a dose effect
or a therapeutic ceiling by the safety concern remain unclear. In ARDS models
of rodents, the effective administration dose is about 20~30 × 106
cells/kg [22]. And in clinical applications above, the dose of MSCs ranged from
1 to 10 × 106 cells/kg. As many believe that higher doses will give
enhanced or prolonged response, besides higher dose in the phase 1 trial by JG
Wilson et al. was well tolerated and seemed to have more efficiency [11], the
phase 2 study will use the high dose of 10 × 106 cell/kg [23], which
results will be promising. And perhaps equally importantly, since the kinetics
of an MSC graft is transient with a half-life of approximately 24 h [24], it is
unclear whether a second infusion of MSCs is needed.
The pathologic hallmark of ARDS is diffuse alveolar damage [1],
but it is difficult to distribute the cells uniformly in lung tissue by
intratracheal injection, and the intravenous route of a large amount of cell
suspension may be more practical for clinical application in hypoxemic ARDS
patients. However, for patients with bacterial infection, the intrapulmonary
delivery of MSCs may be more efficient to enhance their antimicrobial activity
through the secretion of antimicrobial peptides. Besides,
Qin et al. found that MSCs delivered by intra-pleural delivery can prolong MSCs
survival to at least one month [25]. Although promising, the optimal delivery
route needs further investigation [22].
Besides, there are challenges in cell preparation including production
and cryopreservation methods which may induce changes in cells function. In one
study the viabilities of the given cells were only about 56% [11]. Furthermore,
cell viability assays couldn’t provide data regarding
the potency of the cells. It was recommended that the cell lysates of MSC
should be tested for potency by measuring some paracrine factors [2]. And it is
necessary to establish a quantitative criterion for quality control of stem
cells therapy, in cell characterization, cell viability and potency, bacterial
and viral detection, etc.
STUDY OUTCOMES
Along with the complicated mechanisms of stem cell therapy, we need
more comprehensive evaluations on the impact of MSCs treatment rather than
mortality only.
Efficacy endpoints proposed in the ongoing phase II clinical trial
exhibited an excellent example [23], in which respiratory efficacy endpoints (LIS,
the PaO2/ FiO2 ratio, arterial blood gas measurement and chest radiograph),
systemic efficacy endpoints (SOFA score, ventilator-free, ICU-free,
vasopressor-free, organ failure free days and 60-day mortality), as well as all
aspects of biologic measurements (inflammation indices, indexes of epithelial/
endothelial injury, analysis on MSCs paracrine activity,
and other main organs injury). For MSCs paracrine activity measurements, in
addition to angiopoietin-1 and keratinocyte growth factor mention in this
study, we suggest that it is better to detect the quantity and function of the
extracellular vesicles produced by stem cells in BAL and serum as well [26,27].
And the follow-up period of this study was about to be extended to 12 months,
which will provide a longer-term effect of MSCs therapy.
CONCLUSION
Though questions and concerns remain, stem cell-based therapies are
undergoing rapid development and offer promise for the treatment of ARDS. We
expect more clinical trials with elaborate experimental design based on support
from basic research, hoping that feasible and effective MSCs therapy can
eventually change the treatment diagram of ARDS.
ACKNOWLEDGEMENT
This study was supported by The National Natural Science Foundation of China key grant (81630001, 81490533), grant (81770075, 81770055, 81500026, 81570028, 81600056), The State Key Basic Research Program project (2015CB553404), Shanghai Science and Technology Committee grant (15DZ1930600/15DZ1930602/16ZR1405700) and Shanghai Municipal Commission of Health and Family Planning (201540370).
1. Force
ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND (2012) Acute
respiratory distress syndrome: the Berlin Definition. JAMA 307: 2526-2533.
2. Laffey
JG, Matthay MA (2017) Fifty Years of Research in ARDS. Cell-based Therapy for
Acute Respiratory Distress Syndrome. Biology and Potential Therapeutic Value.
Am J Respir Crit Care Med 196: 266-273.
3. Pittenger
MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R (1999) Multilineage potential of
adult human mesenchymal stem cells. Science, 284: 143-147.
4. Wang
Y, Chen C (2016) The Mechanism of MSCs Therapy in Acute Respiratory Distress
Syndrome. Journal of Clinical Respiratory Diseases and Care 2.
5. Chang
Y, Park SH, Huh JW, Lim CM, et al. (2014) Intratracheal administration of
umbilical cord blood-derived mesenchymal stem cells in a patient with acute
respiratory distress syndrome. J Korean Med Sci 29: 438-440.
6. Simonson
OE, Mougiakakos D, Heldring N, Bassi G, Johansson HJ, et al. (2015) In Vivo
Effects of Mesenchymal Stromal Cells in Two Patients With Severe Acute
Respiratory Distress Syndrome. Stem Cells Transl Med 4: 1199-213.
7. Mirzaei
H, Sahebkar A, Sichani LS, Moridikia A, Nazari S, et al. (2018) Therapeutic
application of multipotent stem cells. J Cell Physiol 233: 2815-2823.
8. Lalu
MM, McIntyre L, Pugliese C, Fergusson D, Winston BW, et al. (2012) Safety of
cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and
meta-analysis of clinical trials. PLoS One 7: e47559.
9. Liu
WW, Yu W, Chen JY, Ye GX, Liu YM, et al. (2012) Effects of human umbilical cord
mesenchymal stem cells in the treatment of paraquat-induced lung injury.
Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 30: 811-815.
10. Zheng
G, Huang L, Tong H, Shu Q, Hu Y, et al. (2014) Treatment of acute respiratory
distress syndrome with allogeneic adipose-derived mesenchymal stem cells: a
randomized, placebo-controlled pilot study. Respir Res 15: 39.
11. Wilson
JG, Liu KD, Zhuo H, Caballero L, McMillan M, et al., Mesenchymal stem (stromal)
cells for treatment of ARDS: a phase 1 clinical trial. Lancet Respir Med 3:
24-32.
12. Trounson
A, McDonald C (2015) Stem Cell Therapies in Clinical Trials: Progress and
Challenges. Cell Stem Cell 17: 11-22.
13. Kendall
JM (2003) Designing a research project: randomised controlled trials and their
principles. Emerg Med J 20: 164-168.
14. Altman
DG (1991) Randomization. Br Med J 302: 1481-1482.
15. Hulley
SB (2007) Designing clinical research. (3rd edn), Lippincott
Williams & Wilkins, Philadelphia, PA.
16. Perl
M, Lomas-Neira J, Venet F, Chung CS, Ayala A (2011) Pathogenesis of indirect
(secondary) acute lung injury. Expert Rev Respir Med 5: 115-126.
17. Calfee
CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, et al. (2014) Subphenotypes
in acute respiratory distress syndrome: latent class analysis of data from two
randomised controlled trials. Lancet Respiratory Med 2: 611-620.
18. Melief
SM, Zwaginga JJ, Fibbe WE, Roelofs H
(2013) Adipose tissue-derived multipotent stromal cells have a higher
immunomodulatory capacity than their bone marrow-derived counterparts. Stem
Cells Transl Med 2: 455-463.
19. Kern
S, Eichler H, Stoeve J, Klüter H, Bieback K (2006) Comparative analysis of
mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose
tissue. Stem Cells 24: 1294-1301.
20. Ma
Q, Ma Y, Dai X, Ren T, Fu Y, et al. (2018) Regeneration of functional alveoli
by adult human SOX9(+) airway basal cell transplantation. Protein Cell.
21. Cao
JP, He XY, Xu HT, Zou Z, Shi XY (2012) Autologous transplantation of peripheral
blood-derived circulating endothelial progenitor cells attenuates
endotoxin-induced acute lung injury in rabbits by direct endothelial repair and
indirect immunomodulation. Anesthesiol 116: 1278-1287.
22. Zhu
YG, Hao Q, Monsel A, Feng XM, Lee JW et al. (2013) Adult stem cells for acute
lung injury: remaining questions and concerns. Respirology 18: 744-756.
23. Liu
KD, Wilson JG, Zhuo h, Caballero L,
McMillan ML, et al. (2014) Design and implementation of the START (STem
cells for ARDS Treatment) trial, a phase 1/2 trial of human mesenchymal
stem/stromal cells for the treatment of moderate-severe acute respiratory
distress syndrome. Ann Intensive Care 4: 22.
24. Parekkadan
B, Milwid JM(2010) Mesenchymal stem cells as therapeutics. Annu Rev Biomed Eng
12: 87-117.
25. Qin
ZH, Xu JF, Qu JM, Zhang J, Sai Y, et al. (2012) Intrapleural delivery of MSCs
attenuates acute lung injury by paracrine/endocrine mechanism. J Cell Mol Med
16: 2745-2753.
26. Matthay
MA (2017) Extracellular Vesicle Transfer from Mesenchymal Stromal Cells
Modulates Macrophage Function in Acute Lung Injury. Basic Science and Clinical
Implications. Am J Respir Crit Care Med 196: 1234-1236.
27. Monsel
A, Zhu YG, Gudapati V, Lim H, Lee JW (2016) Mesenchymal stem cell derived
secretome and extracellular vesicles for acute lung injury and other
inflammatory lung diseases. Expert Opin Biol Ther 16: 859-871.
-
 Table 1
Table 1
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Spine Diseases
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns


