8236
Views & Citations7236
Likes & Shares
Objective: To determine the prevalence of vitamin B12
deficiency in patients with type-2 diabetes mellitus attending secondary care
endocrinology clinic and study the possible factors that might affect vitamin
B-12 serum level.
Design: Retrospective cross-sectional study.
Setting: Salmaniya Medical Complex, Kingdom of
Bahrain.
Methods: From January 2018 to December 2018, 306
patients with type-2 diabetes mellitus were included. Baseline demographic
characteristics, physical and laboratory investigations were retrieved from
electronic medical records. For statistical analysis, Prism (Graph Pad)
software was used.
Results: Of the 306 cases, 62.1% of patients were
female (vs. 37.9 % were male) and the mean age of the patients was 57.6years.
This study found that around 93% (n=284) of patients with type 2 diabetes
mellitus had normal or borderline vitamin B12 levels, whereas vitamin B12
deficiency was noticed in 7% (n=22) of the cases. No significant differences
between these groups were found. Metformin use has been found to be
significantly associated with vitamin B12 deficiency (P=0.0341).
Conclusion: The estimated prevalence of vitamin B12
deficiency in patients with type-2 diabetes mellitus was 7%. Use of metformin
was significantly associated with vitamin B12 deficiency and thus routine
screening should be considered in metformin users, particularly in patients
with neuropathic symptoms.
Keywords: Diabetes mellitus, Vitamin B12 deficiency,
Metformin, Cobalamin deficiency
INTRODUCTION
Vitamin B12, also known as
Cobalamin, is a water-soluble vitamin that is found naturally in animal products
[1]. This vitamin is essential for
nucleic acids synthesis, cellular metabolism mitochondrial metabolism and
neurological functions [2].
Low cobalamin levels may lead to significant
hematological, gastrointestinal and neuropsychiatric complications, but
asymptomatic subjects are not uncommon [1]. Periodic assessment of this vitamin
should be considered in patients with risk factors including prolonged use of
metformin, proton pump inhibitors (PPIs) and advanced age [2]. American
Diabetes Association (ADA), for instance, recommends periodic assessment of
serum B-12 levels in metformin-treated patients, particularly in the presence
of anemia or peripheral neuropathy. Screening for vitamin B12 deficiency is not
recommended in average-risk adults [3].
Cobalamin deficiency is more common in
patients with T2DM not only due to metformin use, but also due to advanced age
and nutritional deficiencies [3,4]. Due to cost-effectiveness, low risk of hypoglycemia
and cardiovascular benefits, metformin is a first-line therapy for the
treatment of T2DM. It is estimated that almost 120 million
patients
Type-2 Diabetes Mellitus (T2DM) is one of the rapidly growing epidemics,
especially in the Eastern Mediterranean and Middle East regions [7]. The
prevalence of disease in Bahrain is reported to be between 14-17% [8] Most of
the patients with T2DM are managed according to the standard guidelines in
Primary Health Care (PHC), however, uncontrolled cases and/or patients with
diabetes-related complications are referred to secondary care mostly at
Salmaniya Medical Complex (SMC) for further management.
In Bahrain, a study was conducted among adult
T2DM patients attending the primary care department diabetic clinic at the
Bahrain Defense Force (Military Hospital) found that the prevalence of low
vitamin B12 level was 43.6% among adults with T2DM patients on metformin [9]. The
aim of this study is to determine the prevalence of vitamin B-12 deficiency
among patients with T2DM, particularly in metformin-users and elderly patients attending
endocrine clinic at SMC.
METHODS
Study design and
participants
This retrospective
cross-sectional study was conducted at SMC in the period between January 2018 and
December 2018. All adults (≥ 18 years) with T2DM were enrolled. Those who have
not had their vitamin B12 levels measured and patient who had gastrectomy were
excluded from the analysis. All T2DM patients who
presented to endocrinology clinics in the first week of every month between
January 2018 and December 2018 were included. The protocol of this study
was reviewed and approved by Secondary Healthcare Research Committee at
Ministry of Health.
Data
collection
Data
collection sheet was developed and used to collect the following data from the
electronic medical records. The primary outcome was vitamin B12 serum levels
while the secondary outcomes were participants’ baseline demographic
characteristics (age, sex and nationality), diabetes control determined by A1C
levels, diabetes medications, presence of underlying of comorbidities, blood
pressure, lipid profile, renal function, thyroid stimulating hormone (TSH) and
vitamin D status were recorded.
Serum vitamin b12 assays
B-12
level of ≤ 148 p mol/L was considered low (deficiency), more than 221 pmol/L
was considered normal and borderline level was considered as serum B-12 level
>148 to ≤ 221 pmol/L [10].
STATISTICAL ANALYSIS
All
data were de-identified in the analysis process using serial numbers. Continuous variables were
expressed as means with 95% confidence interval, while categorical variables
were expressed as frequencies and percentages. Prism (Graph Pad) software was
used for statistical analyses and differences with P value<0.05 were
considered statistically significant. T-test was used to compare between
continuous data. Differences, associations and interactions between categorical
variables were analysed using the chi-square test and Fisher’s exact test.
RESULTS
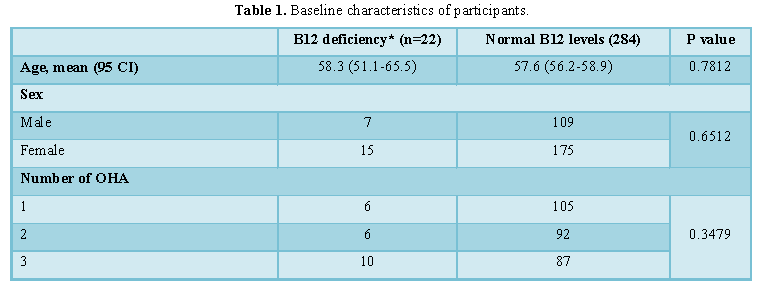
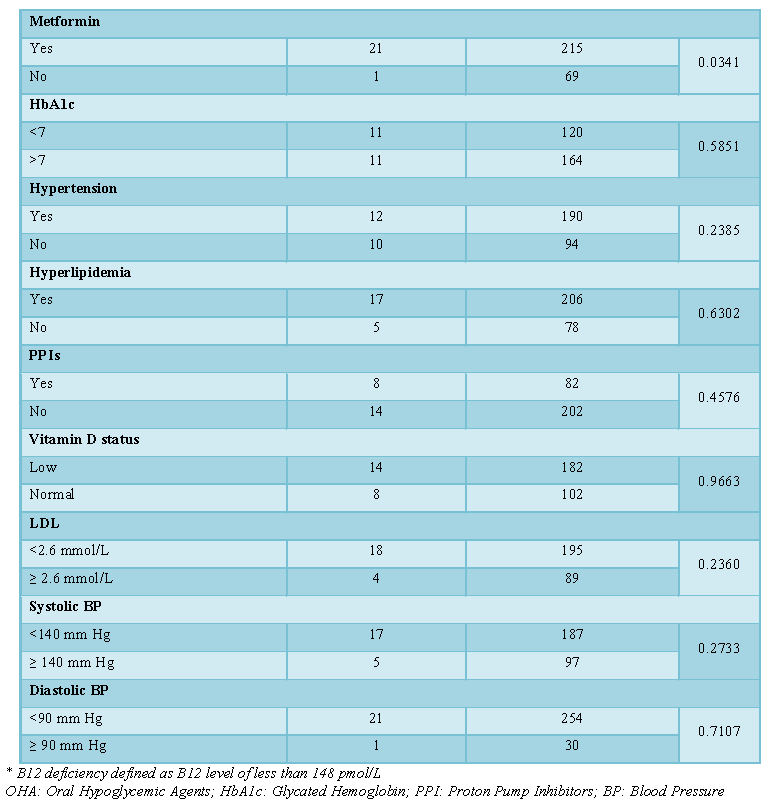
Baseline characteristics
A total of 387 records were reviewed but
serum B-12 levels were available in 306 cases only. The baseline
characteristics of the participants are shown in Table 1. Approximately two-third of the patients were female
(62.1%; n=190), had hypertension (66.0%; n=202), hyperlipidemia (72.9%; n=223)
and low vitamin D levels (64.1%; n=196).
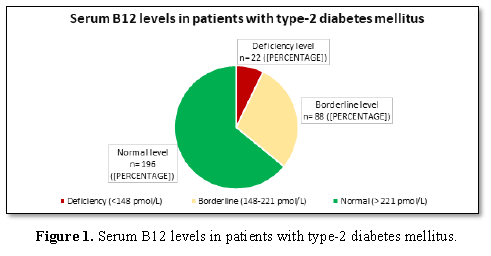
B12 serum
status
The vast majority of the patients had normal
or borderline serum B12 levels (n=284; 94%) and only 7% (n=22) of the patient
had low B12 levels (Figure 1). No significant
differences were found between patients with low and those with normal B12
results except for being on metformin (P=0.0341).
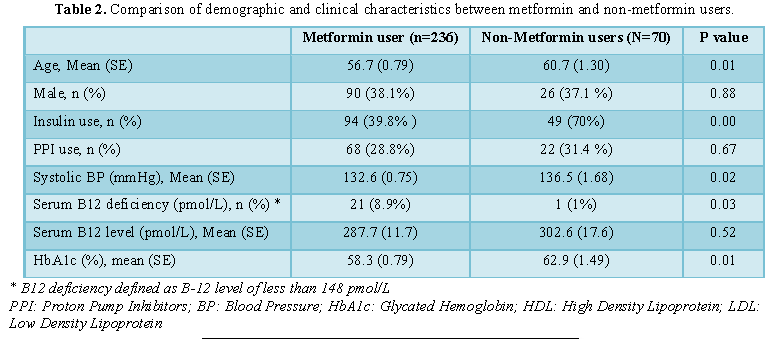
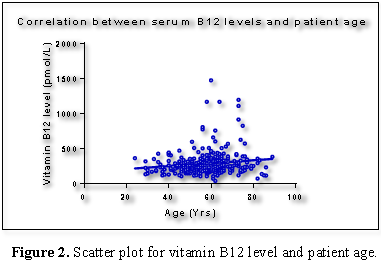
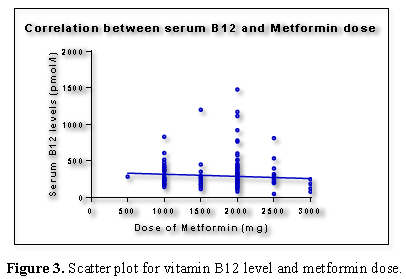
Serum B12
levels, patient age, metformin use and dose
There was a weak positive correlation between
the age and serum-B12 levels. Patients who were treated with metformin were
younger (56.7 vs. 60.7 years; P=0.01), had lower HbA1c results (58.3 vs. 62.9;
P= 0.01) and lower systolic BP (132.6 vs. 136.5; P=0.02). No significant
differences between metformin-user and non-metformin users in sex ratio, ALT,
LDL and total cholesterol levels. Most importantly, vitamin B12 deficiency was
significantly associated with metformin use (8.9% vs. 1%; P=0.03). Metformin
users who had low B12 levels were female (71.4%; n=15), using 2000 mg/day
(61.9%; n=13) and had a reasonable A1C<7% (52.4%; n=11) (Table 2 and Figures 2 and 3).
DISCUSSION
The main objectives of the current
study it to determine the prevalence of B12 deficiency and the risk factors for
this condition. Similar to multiple regional observations, our results showed
that the prevalence of B12 deficiency in patients with T2DM was around 7% [11].
While B12 deficiency was more prevalent (43.6%) in the study conducted at Royal
medical services military hospital. This might be partly explained by the
different cut-off points used to define B12 deficiency (300 pmol/L) [12,13]. In
addition, this difference in prevalence could be attributed to the differences in
study population managed at primary care level and those referred to secondary
care specialized endocrinology clinics that tend to have more complications and
less stringent control. Moreover, having higher prevalence of B12 deficiency
among T2DM metformin users should be cautiously interpreted in view of small
number of cases in the non-metformin users in such studies.
Consistent with most of the studies, we
found a statistically significant association between cobalamin deficiency and
metformin use. For example, a systematic review found an increase in the
incidence of B12 deficiency in metformin users compared to non-users [12]. In
another study in Saudi Arabia, the overall prevalence of B12 deficiency among
patients with T2DM was estimated to be 7.8% with statistically significant
higher prevalence among metformin users [13]. However, interestingly, a recent
study conducted in Qatar found comparable serum B12-levels between Metformin
and non-Metformin users with T2DM [13]. Presently, although the exact mechanism
of this association remains unclear, proposed mechanisms include alterations in
small bowel motility, competitive inhibition of B12 absorption and alterations
in intrinsic factor levels [14].
Additionally, the results of the
present study have demonstrated a weak negative correlation between B-12 level
and metformin dose. Such a relationship was also seen and evaluated in some observations.
For instance, a study conducted in Netherlands concluded that higher doses of
metformin were strongly associated with lower cobalamin levels [15]. This
effect was found even in persons at high risk for type 2 diabetes who used
metformin [16]. Studies have reported that PPIs use and patients’ age decrease
the serum level of B12 but this effect was not obvious in this analysis
[17,18].
The clinical significance of B12
deficiency is to be determined particularly in asymptomatic individuals. In
addition, the sensitivity and specificity of current assays and one reading B12
serum level remains limited in excluding or confirming the diagnosis.
Methyl-Malonic Acid levels (MMA) and homocysteine are additional markers that
can be utilised to improve the accuracy of the diagnosis in symptomatic patients
with normal B-12 levels [19,20]. However, none of these tests is specific for the
diagnosis [21].
This study has several strengths. It is
the first study to investigate the prevalence of B12 deficiency in patients
with T2DM in a public hospital in Bahrain. The most important parameters were
evaluated and patients with different baseline characteristics were included.
One of the limitations of this study is that some factors that could affect B12
level have not been evaluated. These include duration of metformin use;
duration of diabetes and the presence of underlying gastric pathologies could
not be obtained retrospectively in our setting. Because elevated level of MM Aim
proves the diagnostic accuracy, another limitation was the lack of MMA
measurements.
CONCLUSION
In
conclusion, this study estimates the prevalence of cobalamin deficiency to be
around 7%. Among adults with T2DM, there was a statistically significant
association between metformin use and B12 deficiency. Given the accumulating
evidence associating metformin use to cobalamin deficiency, periodic
measurement of serum B12 should be considered in metformin-users, especially in
the presence of neurological and/or anemia symptoms. Further studies to assess
the feasibility and cost-effectiveness of screening all T2DM and the role of
prophylactic cobalamin in this setting.
FUNDING
The authors declare that they have no funding source.
AUTHOR CONTRIBUTIONS
HT and MA contributed to the study conception and design; HA, RF, RA and
HF collected the data; MA and HA analysed the data and drafted the article. All
authors reviewed the manuscript and approved the final version of this study.
CONFLICT OF INTEREST
Authors declare no conflict of interest.
1.
Oh RC, Brown
DL (2003) Vitamin B12 deficiency. Am Fam Physician 67: 979-986.
2.
Langan RC,
Goodbred AJ (2017) Vitamin B12 deficiency: Recognition and management. Am Fam
Physician 96: 384-389.
3.
Chow BF, Stone
HH (1957) The relationship of vitamin B12 to carbohydrate metabolism and
diabetes mellitus. Am J Clin Nutr 5: 431-439.
4.
Pflipsen MC,
Oh RC, Saguil A, Seehusen DA, Seaquist D, et al. (2009) The prevalence of
vitamin B12 deficiency in patients with type 2 diabetes: A cross-sectional
study. J Am Board Fam Med 22: 528-534.
5.
Ahmed MA,
Muntingh G, Rheeder P (2016) Vitamin B12 deficiency in metformin-treated type-2
diabetes patients, prevalence and association with peripheral neuropathy. BMC
Pharmacol Toxicol 17: 44.
6.
American
Diabetes Association (2019) Pharmacologic approaches to glycemic treatment:
Standards of medical care in diabetes. Diabetes Care 42: S90-S102.
7.
Kharroubi AT,
Darwish HM (2015) Diabetes mellitus: The epidemic of the century. World J
Diabetes 6: 850-867.
8.
International
Diabetes Federation (2013) IDF Diabetes Atlas. 6th Edn. Brussels,
Belgium.
9.
Nasser F,
Islam T (2018) Association of vitamin B12 and metformin in type II diabetes
patients in Bahrain. J Diabetes Metab 9: 796.
10.
Reinstatler L,
Qi YP, Williamson RS, Garn JV, Oakley GP Jr. (2012) Association of biochemical
B12 deficiency with metformin therapy and vitamin B12 supplements: The National
Health and Nutrition Examination Survey, 1999-2006. Diabetes Care 35: 327-333.
11.
Alharbi TJ,
Tourkmani AM, Abdelhay O, Alkhashan HI, Al-Asmari AK, et al. (2018) The
association of metformin use with vitamin B12 deficiency and peripheral
neuropathy in Saudi individuals with type 2 diabetes mellitus. PLoS One 13:
e0204420.
12.
Niafar M, Hai
F, Porhomayon J, Nader ND (2015) The role of metformin on vitamin B12
deficiency: A meta-analysis review. Int Emerg Med 10: 93-102.
13.
Elhadd T,
Ponirakis G, Dabbous Z, Siddique M, Chinnaiyan S, et al. (2018) Metformin use
is not associated with B12 deficiency or neuropathy in patients with type 2
diabetes mellitus in Qatar. Front Endocrinol 9: 248.
14.
Kibirige D,
Mwebaze R (2013) Vitamin B12 deficiency among patients with diabetes mellitus:
Is routine screening and supplementation justified? J Diabetes Metab Disord 12:
17.
15.
Beulens JW,
Hart HE, Kuijs R, Kooijman-Buiting AM, Rutten GE (2015) Influence of duration
and dose of metformin on cobalamin deficiency in type 2 diabetes patients using
metformin. Acta Diabetol 52: 47-53.
16.
Aroda VR,
Edelstein SL, Goldberg RB, Knowler WC, Marcovina SM, et al. (2016) Long-term
metformin use and vitamin B12 deficiency in the Diabetes Prevention Program
Outcomes Study. J Clin Endocrinol Metab 101: 1754-1761.
17.
Heidelbaugh JJ
(2013) Proton pump inhibitors and risk of vitamin and mineral deficiency:
Evidence and clinical implications. Ther Adv Drug Saf 4: 125-133.
18.
Qorraj-Bytyqi
H, Hoxha R, Sadiku S, Bajraktari IH, Sopjani M, et al. (2018) Proton pump
inhibitors intake and iron and vitamin B12 status: A prospective comparative
study with a follow up of 12 months. Open Access Maced J Med Sci 6: 442-446.
19.
Stabler SP (2013) Vitamin B12 deficiency. N
Engl J Med 368: 149-160.
20.
Joosten E, van
den Berg A, Riezler R, Naurath HJ, Lindenbaum J, et al. (1993) Metabolic
evidence that deficiencies of vitamin B12 (cobalamin), folate and vitamin B6
occur commonly in elderly people. Am J Clin Nutr 58: 468-476.
21.
Oberley MJ,
Yang DT (2013) Laboratory testing for cobalamin deficiency in megaloblastic anemia. Am J Hematol 88:
522.
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Spine Diseases
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Cell Signaling & Damage-Associated Molecular Patterns


