695
Views & Citations10
Likes & Shares
Background: Clinical signs and symptoms cannot distinguish accurately between viral and group A beta-hemolytic streptococcus pharyngotonsillitis and a significant proportion of those seen especially in general practice received antibiotics not recommended by guidelines, an inadequate length of treatment or no prescription.
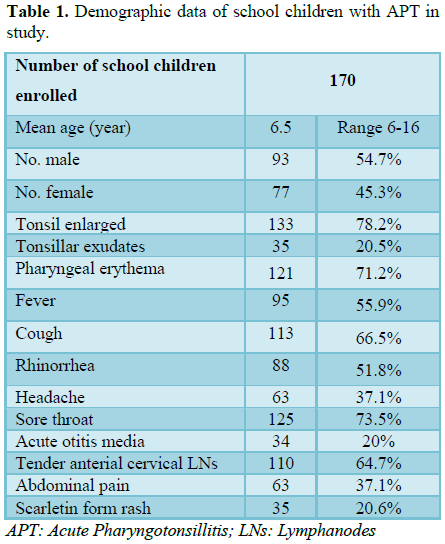
Material and methods: One hundred and seventy, 6 to 16 years old school children suffered from pharyngotonsillitis were recruited in this study. Throat swab culture with blood agar culture medium was used in all participants and amoxicillin/clavulanate 40 mg/kg/day administered twice daily for 10 days if the culture result showed GAS infection.
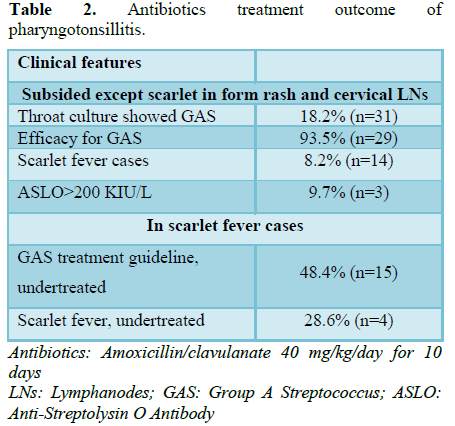
Results: 18.2% (n=31) schoolchildren showed Streptococcus pyogen growth in the throat culture and 14 children (45.2%) of those present with clinical features of scarlet fever. The efficacy of amoxicillin/clavulanate treatment was effective and safety in 93.5% (n=29) in group A streptococcal pharyngotonsillitis. However, among the 31 cases, there were 15 cases not coming back to follow up and 4 of them were scarlet fever cases.
Conclusion: This study confirms that the administration of amoxicillin/clavulanate 10 days eradicated group A streptococcal pharyngotonsillitis effectively, but most of the patients did not follow the treatment guideline and inadequate length of treatment is the key factors of increasing carrier rate.
Keywords: Beta-hemolytic, Streptococcal pharyngotonsillitis, Amoxicillin/clavulanate
INTRODUCTION
MATERIALS AND METHODS
We analyzed retrospectively the data on microbiological studies and throat swab culture done, and data on prescribing of antibiotics, of 170 children visit our outpatient clinic for pharyngotonsillitis from September 1, 2016 to August 31, 2017. The schoolchildren enrolled in the study were 6 to 16 years of age. Throat swab culture with blood agar culture medium was used in all participants for microbiological agent detection. An amoxicillin/clavulanate 40 mg/kg/day were given twice daily for 10 days if the culture result showed GAS infection (Table 1).
RESULTS
After the clinical diagnosis of pharyngotonsillitis, throat swab culture for GAS identification was done in all cases. Thirty one in one hundred seventy (18.2%) APT children have GAS infection, among them 45.2% (n=14) has present with scarlet fever clinical features. Antibiotics were started and the efficacy of amoxicillin/clavulanate treatment was effective and safety in 93.5% (n=29) of GAS infection. Anti-streptolysin O antibody follow up showed 3 cases increased higher than 200 KIU/L but patient did not have any complications during that time. Among the 31 GAS infected cases, there were 15 cases did not coming back follow up and 4 of them were the scarlet fever cases (Table 2).
DISCUSSION AND CONCLUSION
Group A streptococcus is the most frequently identified bacterium in children with APT, although group B, C, F and G have also been associated with APT. In Leao [6] study, higher APT incidence was observed in the female gender and tonsillar exudates were observed with group A and C predominant. To assess the utility of clinical features for diagnosis of APT with GAS in pediatrics with throat cultures showed that clinical presentation should not be used to confirm APT because its performance as a diagnostic test is low. It also pointed out that coryza absence, conjunctivitis absence; pharyngeal erythema, pharyngeal exudate, and tonsillar swelling were significantly associated with streptococcal pharyngotonsillitis. The highest clinical score, characterized by coryza absence, pharyngeal exudate, and pharyngeal erythema had 45.6% sensitivity, 74.5% specificity, and a likelihood ratio of 1.79 for streptococcal pharyngotonsillitis [7]. All guidelines agree that narrow-spectrum antibiotic is the first choice of antibiotic for the treatment of APT and penicillin and amoxicillin are the first choice antibiotics in the case of a child with the proven presence of GAS infection, however, the number of orally administered doses and 10 days of therapy considerably lower the compliance [3,8]. In opposite, the length of the treatment was the aspect found to be most deficient in lot of APT patients [9]. As mentioned above, some European guidelines only recommend antibiotic treatment in certain high-risk patients, while many others, including all American; still advise antimicrobial treatment for all children with GAS pharyngitis, given the severity and re-emerging incidence of complications. Moreover, the severity and the possibly increasing incidence of complications in school-aged children suggests that testing and treating proven GAS pharyngitis can still be beneficial [10].
Molecular analysis of GAS isolated from patients with APT showed macrolide resistance mediated by themef(A) gene and due to the high levels of macrolide resistance observed, GAS isolates from individuals with penicillin allergies need be isolated and their antimicrobial susceptibility tested, rather than automatically giving the patient a macrolide [11]. The inadequate penetration of penicillins into the tonsillar tissues and tonsillar surface fluid and microbiologic interactions between GAS and other pharyngotonsillar bacterial flora can account for their failure in eradicating GAS pharyngotonsillitis. These interactions include the presence of beta-lactamase producing bacteria (BLPB) that shield GAS from penicillins [12]. Another current study proposed that the presence of ß-lactamase in non-typeable Hemaophilus influenza and Moraxella catarrhalis produced from outer membrane vesicles, which may contribute to the treatment failures seen in GAS pharyngotonsillitis [13]. Thus, administration of amoxicillin/clavulanate can eradicate both aerobic and anaerobic BLPB, as well as GAS and that is why we chose to use this antibiotic in the study. In this current study, we confirmed administered amoxicillin/clavulanate 40 mg/kg/day for 10 days can eradicate GAS pharyngotonsillitis effectively. However, routine throat culture for GAS in children with APT is necessary since 18.2% of the patients were found to have GAS infection and anti-streptolysin O antibody was found increased higher than 200 KIU/L in 3 cases, thus, complications might occur. The other important finding is that most of the patients did not come back to follow up even we proved GAS infection and inadequate length of treatment is the critical point of increasing the carrier rate. In the future study, multi-centers, large number of participants and long-term complications follow up should be applied.
1. Harrist A, Van Houten C, Shulman ST, Van Beneden C, Murphy T (2016) Notes from the field: Group A streptococcal pharyngitis misdiagnoses at a rural urgent-care clinic — Wyomain, March 2015. MMWR Morb Mortal Wkly Rep 64: 1383-1385.
2. Di Muzio F, Barucco M, Guerriero F (2016) Diagnosis and treatment of acute pharyngitis/tonsillitis: A preliminary observational study in general medicine. Eur Rev Med Pharmacol Sci 20: 4950-4954.
3. Chiappini E, Regoli M, Bonsignori F, Sollai S, Parretti A, et al. (2011) Analysis of different recommendations from international guidelines for the management of acute pharyngitis in adult and children. Clin Ther 33: 48-58.
4. Shetty A, Mills C, Eggleton K (2014) Primary care management of group A streptococcal pharyngitis in Northland. J Prim Health Care 6: 189-194.
5. de Jongh E, Opstelten W (2015) Revision of the Dutch College of general practitioners practice guideline ‘Acute sore throat’. Ned Tijdschr Geneeskd 159: A9456.
6. Leao SC, Leal IO, Recha HM, Rodrigues TM (2015) Evaluation of cytokines produced by ß-hemolytic streptococcus in acute pharyngotonsillitis. Braz J Otorhinolarynol 81: 402-407.
7. Barbosa Junior AR, Oliveira CD, Fonres MJ, Lasmar LM, Camargos PA (2014) Diagnosis of streptococcal pharyngotonsillitis in children and adolescents: Clinical picture limitations. Rev Paul Pediatr 32: 285-291.
8. Bottaro G, Biasci P, Lo Giudice M, Mele G, Montanari G, et al. (2012) 5 days cefaclor vs. 10 days amoxicillin/clavulanate in the treatment of childhood streptococcal pharyngitis. Data from a randomized clinical trial. Minerva Pediatr 64: 341-346.
9. Duran Fernandez-Feijoo C, Marques Ercilla S, Hernandez-Bou S, Trenchs Sainz de la Maza V, García García JJ, et al. (2010) Antibiotic prescribing in a pediatric emergency department. An Pediatr (Barc) 73: 115-120.
10. Van Brusselen D, Vlieghe E, Schelstraete P, De Meulder F, Vandeputte C, et al. (2014) Streptococcal pharyngitis in children: To treat or not to treat? Eur J Pediatr 173: 1275-1283.
11. Wajima T, Chiba N, Morozumi M, Shouji M, Sunaoshi K, et al. (2014) Prevalence of macrolide resistance among group A streptococci isolated from pharyngotonsillitis. Microb Drug Resist 20: 431-435.
12. Brook I (2013) Penicillin failure in the treatment of streptococcal pharyngotonsillitis. Curr Infect Dis Rep 15: 232-235.
13. Schaar V, Uddback I, Nordstrom T, Riesbeck K (2014) Group A streptococci are protected from amoxicillin-mediated killing by vesicles containing ß-lactamase derived from Hemophilus influenza. J Antimicrob Chemother 69: 117-120.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- International Journal of Diabetes (ISSN: 2644-3031)
- Chemotherapy Research Journal (ISSN:2642-0236)


