899
Views & Citations10
Likes & Shares
Hemangiomas are common neoplasms in the head and neck area in the pediatric age. They represent 2-3% of tumors. Its presentation in the nostril is rare. We present a clinical case of an adult woman who presented nasal obstruction associated with watery rhinorrhea. The computed tomography and magnetic resonance imaging showed tumor of total occupation of the nasal cavity without infiltration of adjacent structures. Complete exeresis was performed under video endoscopy vision.
Keywords: Lobular hemangioma, Vascular nasal tumor
INTRODUCTION
Hemangiomas are benign neoplasms in the head and neck area in the pediatric age; however, they are very rare in the rhinosinusal área [1]. The inferior turbinate, the vomer, the perpendicular lamina of the ethmoid and the maxillary sinus can affect the nasal cavity. They are slow growing, so clinically they are silent at the beginning, as they increase in size they cause deformity and nasal obstruction, depending on the site of origin. Epistaxis, although frequent, is not always the cardinal symptom. The diagnosis is based on clinical suspicion and computed axial tomography, which reveals the existence and characteristics of bone lesions and nuclear magnetic resonance that helps determine the extent of them. Biopsy under endoscopic vision is a useful tool in case of diagnostic doubt. Some authors propose the use of steroids as medical treatment [2,3]. In 5-10%, resection can be performed endoscopically and/or combined externally. In those large tumors, embolization is recommended, prior to surgery [4]. Given the rarity of its presentation in the rhinosinusal area, we present the following clinical case.
CLINICAL CASE
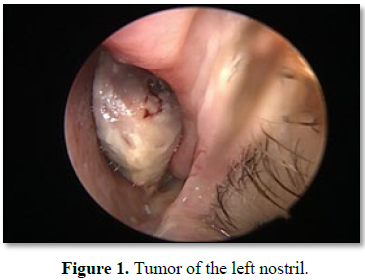
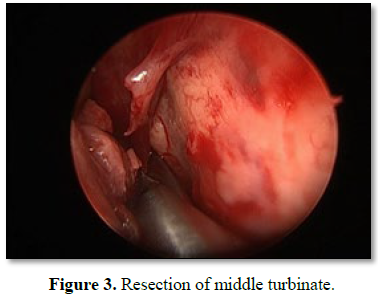
A 57 year old woman, with no relevant history, consulted for a permanent nasal obstruction of the left nostril of 3 months of evolution, associated with watery rhinorrhea. The anterior rhinoscopy shows a tumor that occupies the entire nasal fossa. Fibroscopy shows a lesion that extends along the entire nasal cavity, with nasal septum mucosa of normal appearance, without displacement thereof, free cavum (Figure 1). Computed axial tomography without contrast and nuclear magnetic resonance with facial mass contrast is requested, which informs lesion that occupies the entire left nasal fossa without invasion of the nasal septum, associated with partial occupation of the left maxillary sinus and anterior ethmoid (Figure 2). Under general anesthesia, total tumor resection is performed, including middle turbinate under video endoscopic vision with 30° optic (Figure 3). During the procedure, profuse bleeding of the sphenopalatine artery was observed, which was controlled with electrocoagulation. The postoperative pathological anatomy reported: Lobular hemangioma.
The post-operative evolution was satisfactory, nasal lavages were performed with saline, several times a day for 3 weeks, no immediate or late nasal bleeding was evident. Control was carried out at 10 months (Figure 4).
DISCUSSION AND CONCLUSION
Hemangiomas are the most frequent tumors of childhood. Approximately 60% is located in the head and neck. The nasosinus hemangiomas, unlike the rest, appear in adulthood, so they compress and destroy nearby structures [5]. The most common symptoms when located in the nasal region are epistaxis and nasal obstruction. We must perform the differential diagnosis with other tumors typical of the rhinosinusal cavities, both benign and malignant. Axial computed tomography and nuclear magnetic resonance define the extension and possible involvement of neighboring structures and also contribute differential diagnosis with vascular malformations. Arteriography is indicated on rare occasions; It is done in cases where, due to an excessive size of the lesion for the surgical approach [6,7]. The diagnosis of certainty is given by the incisional biopsy when the location is accessible and excisional during the surgical act. Here are a variety of treatments. Among the non-invasive ones, we find corticosteroids and interferon alfa-2, whose results are acceptable but not without side effects. Among the invasive treatments, the surgical one is the one of choice. The approach must be adapted to the location and size of the tumor [8].
1. Raboso E, Rosell A, Plaza G, Mart´ınez-Vidal A (1997) Haemangioma of the maxillary sinus. J Laryngol Otol 111: 638-640.
2. Jammal H, Barakat F, Hadi U (2004) Maxillary sinus cavernous hemangioma: A rare entity. Acta Otolaryngol 124: 331-333.
3. Shikhani A, Shehadi S (1986) Surgical treatment of giant hemangiomas of the head and neck. Otolaryngol Head Neck Surg 94: 113-122.
4. Biller H, Krespy Y, Soom P (1982) Combined therapy for vascular lesions of the head and neck with intra-arterial embolization and surgical excision. Otolaryngol Head Neck Surg 90: 37-42.
5. Kim HJ, Kim JH, Kim JH, Hwang EG (1995) Bone erosion caused by sinonasal cavernous hemangioma: CT findings in two patients. AJNR 16: 1176-1178.
6. Moore SL, Chun JK, Mitre SA, Som PM (2001) Intraosseous hemangioma of the zygoma: CT and MR findings. Am J Neuroradiol 22: 1383-1385.
7. Kanazawa T, Inou R, Ohta Y, Watanabe Y, Iino Y (2008) Maxillary haemangioma succesfully resected by endoscopic approach. J Laryngol Otol, pp: 1-3.
8. Jammal H, Barakat F, Hadi U (2004) Maxillary sinus cavernous hemangioma: A rare entity. Acta Otolaryngol 124: 331-333.


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- International Journal of Diabetes (ISSN: 2644-3031)


