1136
Views & Citations136
Likes & Shares
One of
the priorities of dentistry is to lower the incidence of oral halitosis.
Malodor is a social concern for an individual and an alarm to unhealthy
lifestyle. It is caused by various oral and extra oral etiologies.
Psycho-physiological stress like menstruation, is one of the common phenomena
among human race, leading to many changes in the body, has also been suggested
in the literatures to be a predisposing factor for the production of volatile
sulfur compounds. A three months cross-sectional study among patients attending
the out-patient Department of Dental Institution in Mysuru was performed. Among
31 participants having menstrual cycle at the time of clinical evaluation,
67.7% had low organoleptic scores while 32.3% had high organoleptic scores.
Conclusion: There was a statistical significant
difference seen in between mean salivary flow and tongue coating with severity
of oral malodor. But there was no significant association between
Psychophysiological Stress and oral halitosis. This could be because of lesser
sample of participants having menstruation involved in the study.
It is
recommended to further conduct various longitudinal and experimental studies
for assessing the causal and scientific relationship, respectively.
Keywords: Oral malodor, Psychophysiological stress,
Salivary flow rate, Menstrual cycle
INTRODUCTION
One of the
major concerns of the human population is oral halitosis, making it the third
most frequent reason for seeking dental aid [1]. Halitosis is a term originated
from the combination of Latin word “halitus” (breathe) with a Greek suffix
“osis” (result of a pathologic process) [2]. Although, every individual
experiences bad breathe occasionally, persistent oral malodor affects at least
50% of the population [3]. Unfortunately, it is to be taken in notice that there
are no elaborated literatures in India regarding prevalence of
normative oral malodor.
Stress has
been also suggested to be a contributory factor in the development of bad
breath [4]. There are evidences which explain psychophysiological differences (like
heart rate patterns) in stress reactivity across the menstrual cycle [5].
Studies have shown that the level of volatile sulfur compounds (VSC) was higher
in menstruation in comparison with other phases like follicular and
pre-menstruation [6-8]. There are sex hormones like ß-estradiol whose effects
were seen on oral mucosa in women [9] and is associated with halitosis [10]. It
can also disturb conditions in the oral cavity through changes in salivary flow
(i.e., may induce hyposalivation). Hyposalivation can alter levels of
antibacterial salivary secretory immunoglobulin A (sIgA) and lactoferrin, which
could promote the accumulation of microorganisms and thereby facilitate the
production of VSC. Past Literature reveals the assumptions that fluctuation in
hormonal variations during different phases of menstrual cycles can influence
anxiety and stress, which in turn affect psychiatric symptoms such as oral
dryness feeling and eventually can increase the VSC [10]. Anxiety and stress
could have effect on sympathetic system activation and then the composition of
saliva [11]. Although, these effects could
Owing to the scarcity of the
literature in the Indian context, the present study was undertaken to assess
the relationship between psycho-physiological stress and oral halitosis using
organoleptic method among adult patients attending a dental institution in
Mysore city, India.
MATERIALS AND METHODOLOGY
The present
descriptive cross-sectional study was undertaken over a period of three months
(May and July 2015) on adult patients attending a dental institution in Mysore
city, India
Prior to the study, ethical clearance was obtained from the
Institutional Ethical Committee, JSS Dental College and Hospital, Mysuru in
accordance with the World Medical Association Declaration of Helsinki 2008, written
informed consent was obtained from
each of the study participants.
A specially
designed structured proforma was used for recording all relevant information
that included demographic details, psycho-physiological stress – tongue
coating, salivary flow rate and oral halitosis. There were other factors like
oral hygiene habits, deleterious habits and oral health status included too in
order to nullify the effects of confounding factors.
A clinical evaluation sheet included the
recording of following parameters: Tongue coating using Winkel Tongue Coating
Index (WTCI) [13]. Unstimulated salivary flow rate [14]. Halitosis using organoleptic
method [15].
Training and
calibration of the examiner:
The clinical examination and measurement of oral halitosis score was carried
out by a single investigator. Prior to the commencement of the study, training
and calibration of the investigator was carried out using Carranza method [16]. The inter-examiner reliability was
found to be good with a Cohen’s Kappa coefficient value of 0.8.
Intra-examiner
calibration: This
was performed by a single investigator on 10 participants in the afternoon
session in the month of April 2015. The participants were examined by the
investigator for plaque, gingival status, tongue coating and oral halitosis
using plaque index, gingival index, tongue coating index and organoleptic
scoring respectively using sterile instruments under adequate illumination. The
second examination of the same 10 participants was carried out in another
afternoon session two days after the baseline examination. The consistency with
regard to organoleptic scoring was satisfactory with the Kappa value of 0.78.
And also was the same for, plaque index as kappa value of 0.69, gingival index
kappa value of 0.72 and winkel’s tongue coating index kappa value of 0.67,
showing a substantial agreement of consistency.
PILOT STUDY
In April 2015, a pilot study was
undertaken on 10 participants to test the feasibility of the protocol, identify
any organizational and technical problems, to eliminate difficulties or
ambiguities in wording of the questionnaire and to test the validity and
reliability of the questionnaire.
Eligibility criteria
Participants who fulfilled the following
eligibility criteria were recruited through a convenience sampling technique
and were not a part of the final study.
Inclusion criteria:
·
Patients attending
out-patient department of college
·
More than 18 years
·
Willing to participate in
the study
·
Permanent dentition
·
Minimum of 20 natural teeth present
Exclusion criteria:
·
Minor and medically compromised
patients (debilitating conditions)
·
Who cannot read and
understand either of Kannada or English languages
·
Undergone already any treatment like oral
prophylaxis 1 month back or undergoing any orthodontic corrections, acute pain
therapies
Sample size estimation
Considering 50% prevalence of halitosis in
patients, 95% confidence interval and 5% of precision (d), the sample size was
calculated to be 500 among which 246 female patients were considered to analyse
the relationship between the physiological stress and oral halitosis.
Sampling design and
methodology
The study participants were selected using
convenience sampling technique to enable ease of data collection. Any
participant willing to enroll in the study attending the outpatient department of
the dental institution was involved.
Administration of
the questionnaire
The study proforma was self-administered to
those subjects who were found eligible for inclusion. However, the investigator
provided brief instruction to the participants before they started filling the
proforma. The subjects took 10-15 min to fill up the questionnaire following
which they were subjected to clinical examination.
RESULTS
The present study was conducted among 500 participants, who fulfilled the eligibility criteria and consented to participate in the study constituted the study sample. We are considering here the female adult population (n=245) among which only 31 patients had presence of menstruation.
Distribution of
age among females in relation to presence of menstrual
cycle
The 245 female participants were asked for
the presence of menstrual cycle at that point of time and 12.7% (n=31) of
females reported yes. The majority of the females (15.6%) were below 35 years
(n=28). Rest were 3.7% (n=1) in the age group of 35-45 years and 5.1% (n=2)
above 45 years reported for the presence of menstrual cycle. There was a
statistical significance (p=0.001) between the menstrual cycle and age groups
of the study participants (Graph 1).
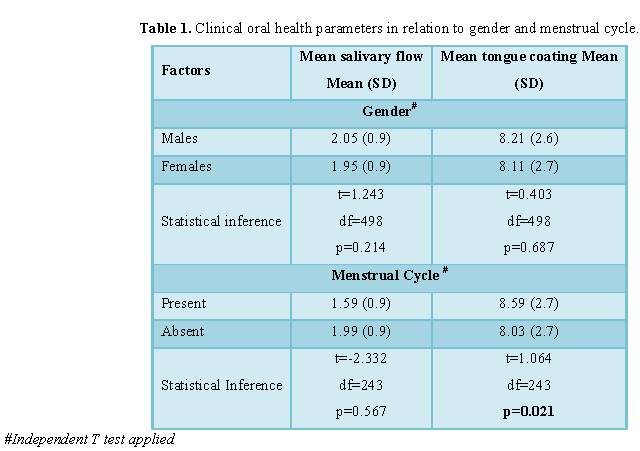
Clinical oral health parameters in relation to various
menstrual cycles
Gender: Independent samples t-test was
applied for comparing various mean scores of clinical parameters in relation to
gender.
Mean salivary flow of study participants in
relation to gender was 2.0 ± 0.9 among which males had salivary flow of 2.05 ±
0.9 and females had 1.95 ± 0.9, showing no statistical significance (p=0.214).
The mean tongue coating index score in
relation to gender was 8.16 ± 2.6. Males had mean tongue coating index score as
8.21 ± 2.6 and females had 8.11 ± 2.7. No statistical significance (p=0.687)
present between gender and mean tongue coating index (Table 1).
Menstrual cycle: Independent samples t-test was
applied for comparing various mean scores of clinical parameters in relation to
menstrual cycle (present/absent).
The mean individual scores salivary flow and
tongue coating indices among the participants who had menstrual periods at that
time were 1.59 ± 0.9, 8.58 ± 2.7, respectively. Whereas, the participants who
claimed absence of menstruation at that point of time had mean individual
scores of salivary flow and tongue coating indices as 1.99 ± 0.9 and 8.03 ± 2.7,
respectively, showing a decrease in all the parameters. There were no
statistical significant difference seen between menstrual cycle and mean
salivary flow (p=0.567) whereas mean tongue coating showed a statistical
significance present between the groups (p=0.021) (Table1).
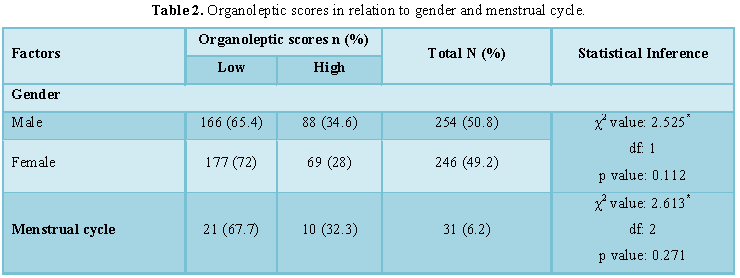
Organoleptic scores in relation to gender and menstrual cycle: The organoleptic scores were
dichotomized as (low and high oral malodor) having low comprised of absent,
slight and moderate organoleptic scores of Rosenberg et al. [15] and high
comprising strong and severe scores.
Chi square test is applied for finding the
prevalence of oral malodor.
Gender: Males (50.8%) were seen with
slightly greater percentage of malodor than females (49.2%). Among males 65.4%
(n=166) had low oral malodor and 34.6% had high oral malodor. Whereas, in
females 72 %( n=177) had low oral malodor and 28% (n=69) had high oral malodor.
There was no statistical significance (p=0.112) seen between the groups (Table2).
Menstrual cycle: Among 6.2% (n=31) participants
having menstruation, 67.7% (n=21) had low organoleptic scores and 32.3% (n=10)
having high malodor, showing no statistical significance (p=0.271) between the
groups (Table2).
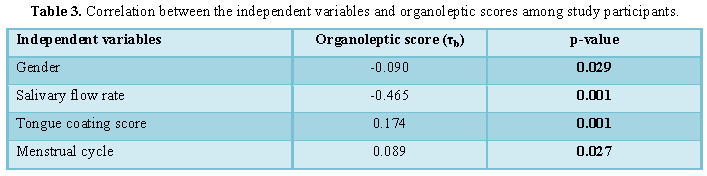
Correlation analysis:
Oral halitosis (organoleptic hedonic scores) was
found to increase in relation to decrease in salivary flow rate and presence of
menstrual cycle. Whereas, oral halitosis is directly proportional to tongue
coating score (Table 3).
Ordinal logistic regression analysis: There was an increase seen in unstimulated salivary flow rate, it was
associated with an increase in organoleptic score having an odds ratio of 0.314
(95% CI, 0.246 to 0.401). This effect was statistically significant (Wald χ2=86.117,
p<0.001).
Also, the increase in the tongue coating
score was associated with an increase in organoleptic scoring having an odds
ratio of 0.989 (95% CI, 1.077 to 1.239). It was statistically significant (Wald
χ2=16.248, p<0.001) too.
The presence of menstrual cycle was
associated with an increase in organoleptic scoring having an odds ratio of
1.414 (95% CI, 0.696 to 2.881) times when compared to female participants not
having menstruation at that point of time of our study. However, the effect was
not statistically insignificant (Wald χ2=0.919, p=0.338) (Table 4).
DISCUSSION
Two forms of stress psychophysiological
(Menstrual cycle) and psychological (self-perceived stress) were considered in
the present study. Among 31 participants having menstrual cycle at the time of
clinical evaluation, 67.7% had low organoleptic scores while 32.3% had high
organoleptic scores. There was a weak positive, statistically insignificant
(p=0.027) correlation (τb=0.089) between menstrual cycle and oral halitosis in
the present study. The presence of menstrual cycle was associated with an
insignificant (p=0.338) increase in organoleptic scoring having an odds ratio
of 1.414. The precise evaluation of the different phases of menstruation would
have resulted in accurate assessment of this association.
However, the decrease in salivary flow rate,
dryness of mouth, stress and anxiety associated with menstruation along with
hormonal changes have all been documented to be predisposing factors for oral
malodor during menstruation [16-18].
There was a study involving 20 female
students to evaluate the association between menstrual cycle and salivary
ß-estradiol as well as with the production of volatile sulfur compounds (VSC)
found mouth odor to be significantly influenced by different phases of
menstruation. The oral malodor although associated with other covariates such
as stresses and dryness of mouth, showing no significant difference in the
salivary flow rate at different phases of menstrual cycle. They concluded that
the exact mechanism on how oral dryness could influence the production of VSC
was not well understood [16]. Also few studies found oral dryness to be
associated with psychological aspects related to pain and anxiety during
menstruation. Anxiety and stress could be influenced by fluctuation of hormonal
changes during different phases of menstrual cycle and affect psychiatric
symptoms such as oral dryness and eventually can increase the VSC. Anxiety and
stress could have effect on sympathetic system activation and composition of
saliva. However, its mechanism was not fully understood [17,18].
One of the observational studies
assessed the changes in VSC levels, clinical parameters and bacterial levels
during menstrual cycle among 10 female subjects with periodontitis and 12
periodontally healthy female subjects. They found that Bleeding on probing
(BOP) significantly increased in the ovulation phase among participants with
periodontitis but not among healthy subjects. The VSC levels in subjects with
periodontitis increased 2.2-fold in the ovulation phase compared with the
follicular phase. In the ovulation phase, VSC levels and BOP were significantly
higher in subjects with periodontitis than in healthy subjects. The number and
salivary levels of prevotella intermedia in subjects with periodontitis were
significantly higher in the ovulation phase than in the follicular phase [19].
CONCLUSION
There was a
statistical significant difference seen in between mean salivary flow and
tongue coating with severity of oral malodor. But there was no significant association
between Psychophysiological Stress and oral halitosis.
The strength of the study is it is single
calibrated trained examiner was present in the study, ruling out the inter
examiner bias. Whereas the limitations of the study are it had only 31 participants
having psychophysiological stress and hence cannot generalize the result. Also,
because of the cross-sectional design of the study, temporal relationships
might have been indicated between stress factors and oral malodor.
It is recommended for a longitudinal approach
assessing stress and oral malodor that could authentically establish causal
relationship. Studies using biochemistry markers, psychological assessment and
other possible explanatory variables should be considered to elucidate the role
of psychological factors in causing odiferous compounds.
1. Ghapanchi J, Darvishi M, Mardani
M, Sharifian N(2012) Prevalence and causes of bad breath in patients attended
Shiraz Dentistry School - A cross sectional study. Elixir Hum Physiol Int J 53:
12051-12054.
2. Kurihara E, Marcondes FK (2002)
Oral concentration of volatile sulphur compounds in stressed rats. Stress 5:
295-298.
3. Bosy A (1997) Oral malodor:
Philosophical and practical aspects. J Can Dent Assoc 63: 196-201.
4. Lima PO, Calil CM, Marcondes FK
(2013) Influence of gender and stress on the volatile sulfur compounds and
stress biomarkers production. Oral Dis 19: 366-373.
5. Olson KC, Carroll HA, Lustyk MKB
(2015) Psychophysiological stress reactivity relationships across the menstrual
cycle. J Hormones 2015: 1-5.
6. Calil CM, Lima PO, Bernardes CF,
Groppo FC, Bado F, et al (2008) Influence of gender and menstrual cycle on
volatile sulphur compounds production. Arch Oral Biol 53: 1107-1112.
7. Queiroz CS, Hayacibara MF,
Tabchoury CP, Marcondes FK, Cury JA (2002) Relationship between stressful
situations, salivary flow rate and oral volatile sulfur-containing compounds.
Eur J Oral Sci 110: 337-340.
8. Tonzetich J, Preti G, Huggins GR
(1978) Changes in concentration of volatile sulphur compounds of mouth air
during the menstrual cycle. J Int Med Res 6: 245-254.
9. Kakoei S, Barkhori F, Mohammadi M,
Mirzazadeh A, Gholamhoseinian A (2012) Influence of menstrual cycle and
salivary ß-estradiol on volatile sulfur compound. J Oral Health Oral Epidemiol
1: 41-45.
10. Meurman JH, Tarkkila L, Tiitinen
AI (2009) The menopause and oral health. Maturitas 63: 56-62.
11. Garrett JR, Ekström J, Anderson LC
(1998) Glandular mechanisms of salivary secretion. 1st Edn. Basle:
Karger S, Publishing.
12. Hamer M, Endrighi R, Venuraju SM,
Lahiri A, Steptoe A (2012) Cortisol responses to mental stress and the
progression of coronary artery calcification in healthy men and women. PLoS One
7: e31356.
13. Winkel EG, Roldán S, Van
Winkelhoff AJ, Herrera D, Sanz M (2003) Clinical effects of a new mouth rinse
containing chlorhexidine, cetylpiridinium chloride and zinc lactate on oral
halitosis. A dual-center, double-blind placebo-controlled study. J Clin
Periodontol 30: 300-306.
14. Speight PM, Kaul A, Melsom RD
(1992) Measurement of whole unstimulated salivary flow in the diagnosis of
Sjogren's syndrome. Ann Rheum Dis 51: 499-502.
15. Rosenberg M, Kulkarni GV, Bosy A,
Mc Cullochm CAG (1991) Reproducibility and sensitivity of oral malodor
measurements with a portable sulphide monitor. J Dent Res 70: 1436-1440.
16. Carranza K, Takei N (2000) Oral
malodor chapter. Clin Periodontol 5: 330-342.
17. Queiroz CS, Hayacibara MF,
Tabchoury CPM, Marcondes FK, Cury JA (2002) Relationship among stressful
situations, salivary flow rate and oral volatile sulphur-containing compounds.
Eur J Oral Sci 110: 337-340.
18. Calil CM, Marcondes FK (2006)
Influence of anxiety on the production of oral volatile sulfur compounds. Life
Sci 79: 660-664.
19.
Kawamoto
A, Sugano N, Motohashi M, Matsumoto S, Ito K (2010) Relationship between oral
malodor and the menstrual cycle. J Periodont Res 45: 681-687.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)
- Journal of Pathology and Toxicology Research
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Advance Research on Alzheimers and Parkinsons Disease
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)



