1940
Views & Citations940
Likes & Shares
Killey and Kay, in 1975, defined oroantral fistula (OAF) as an unnatural communication between the oral cavity and the maxillary sinus resulting most commonly from extraction of teeth. Successful surgical management of oroantral fistula depends on the type of surgical technique implied as well as size and location of the fistula. There are various types of surgical options for the closure of oroantral fistula. Here, we are reporting a case of oroantral fistula in 47 years old male patient, which was successfully managed by buccal advancement flap [Von Rehrmann flap] in M.A. Rangoonwala College of Dental Sciences and Research Centre, Pune.
Keywords: Oroantral communication, Oro-antral fistula, Maxillary sinus, Buccal advancement flap, Von Rehrmann flap
CASE REPORT
A 47 years old male patient visited the department of Oral and Maxillofacial Surgery of our college with the chief complaints of fluid discharge from the upper right back teeth region of jaw since 12 days which was intermittently present. The patient had undergone extraction with upper right first molar, 2 months back as it had poor prognosis.
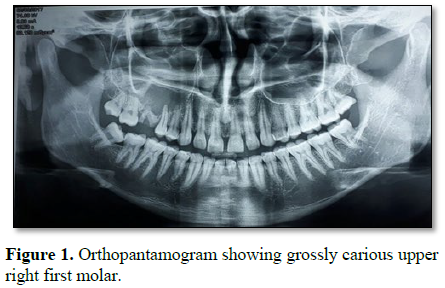
The radiograhic examination which was performed prior to extraction , showed the radiolucency in the right maxillary sinus region and also showed breach in the continuity of floor of the maxillary sinus as shown in Figure 1. The patient's chief complaint was related to the same extraction socket. We examined it clinically. We performed mouth mirror test and cotton wisp test which was found positive. Hence, we advised him radiographic examination.
Figure 1. Orthopantamogram showing grossly carious upper right first molar.
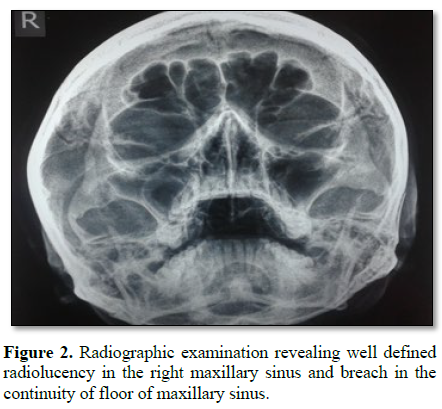
Radiographic examination revealed the presence of breach in the continuity of right side floor of maxillary sinus. This indicated the presence of oroantral fistula in the upper right back teeth region of jaw (Figure 2).
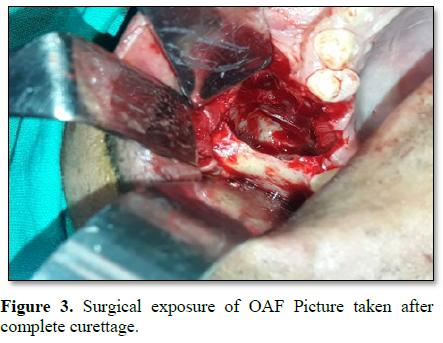
Surgical management of oroantral fistula was planned. All preoperative investigations and measures were done and patient was operated under general anesthesia. The oroantral fistula was located and was exposed. The opening of fistula was located and surgical excision was performed. Surgical curettage and debridement was done and all unhealthy tissue was excised. Figure 3 describes the oroantral fistula after surgical curettage.
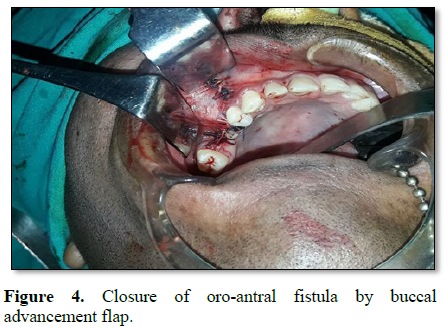
Buccal advancement flap which is also known as Von Rehrmann flap was planned for closure of fistula. An incision was made all around the fistula opening; about 3-4 mm away from it and mucoperiosteum was reflected. From the buccal side of fistula, two divergent incisions were marked, extending towards mucogingival junction. A full thickness mucoperiosteal flap was raised and advanced over the defect. Water-tight closure was performed as shown in Figure 4.
The acrylic stent/plate was placed for one week at the operated as shown in Figure 5. The acrylic stent was designed pre-operatively by taking impression. And this stent was placed to support and protect the operated site, postoperatively. The placement of acrylic stent helps in the stability and proves beneficial for wound support. It also prevents hematoma formation.
The soft tissue specimen was excised from the operated site, i.e., from right maxillary sinus area. This specimen was sent for histopathologic examination. It revealed the presence of dense chronic inflammatory infiltrate interspersed with blood vessel suggestive of the presence inflammatory tissue.
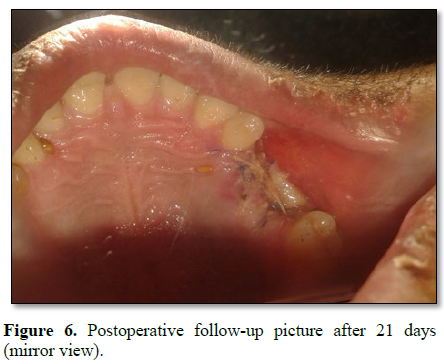
Regular follow-up of the patient was maintained. The Figure 6 shows the postoperative follow-up picture after 21 day which indicates the fistula is completely healed.
DISCUSSION
The pathological connection between the oral cavity and maxillary sinus which takes place because of soft or hard tissue loss which normally separates these compartments is known as oroantral communication (OAC). Oroantral fistula (OAF) is defined as a persistent epithelialized open communication [2]. Killey and Kay, in 1975, defined oroantral fistula (OAF) as an unnatural communication between the oral cavity and the maxillary sinus resulting most commonly from extraction of teeth. Oroantral communication or fistula takes place commonly because of extraction of maxillary molar teeth. It can also occur due to pathological lesions, trauma, neoplasm, iatrogenic injuries and Paget’s disease [4]. Fisulas which are smaller than 5mm in diameter can close spontaneously, whereas larger one requires surgical closure. The success rate percentage is about 90% to 95%, if the primary closure of oroantral fistulas is done in 2 days; whereas it falls to about 67% when closure is done secondary [4]
Various surgical procedures like local or distant flaps and grafting can be used for closure of fistulas. Minor or moderate sized defects can be closed by local flaps. Buccal advancement flap (Von Rehrmann flap), buccal sliding trapezoidal flap (Moczair's flap) and Ashley's flap (Palatal rotational flap) are various types of local flaps which can be used for surgical closure of oroantral fistula (OAF) [1,8,9,13]. Use of buccal fat pad can be done for the closure of OAF which acts as pedicellate graft for the reconstruction of intra-oral defects [2].
In the present case report, oroantral fistula was surgically managed by Von Rehrmann flap. This case was successfully managed in the department of oral & maxillofacial surgery of M.A. Rangoonwala College of Dental Sciences and Research Centre, Pune.
1. Marcantonio C, Palmieri M, Gorga DV, de Oliveira Pereira M, Nícoli LG, et al. (2015) Use of a palatal pedicle flap for closure of an oroantral fistula. RGO, Rev Gaúch Odontol, Porto Alegre 63: 496-501.
2. Junior JCM, Keim FS, Kreibich MS (2008) Closure of oroantral communication using buccal fat pad graft - Case report. Int Arch Otorhinolaryngol 12: 450-453.
3. Nedir R, Nurdin N, Paris M, El Hage M, Najm SA, et al. (2017) Unusual etiology and diagnosis of oroantral communication due to late implant failure. Case Rep Dent 2017: 1-5.
4. Abrahams JJ, Berger SB (1995) Oral-maxillary sinus fistula oroantral fistula: Clinical features and findings on multiplanar CT. AJ 165: 1273-1276.
5. Jadhav KB, Gupta N (2014) Cytological approach for diagnosis of non-healing oroantral fistula associated with candidiasis. J Cytol 31:47-49.
6. Awang MN (1988) Closure of oroantral fistula. Int J Oral Maxillofacial Surg 17: 110-115.
7. Visscher SH, van Minnen B, Bos RR (2010) Closure of oroantral communications: A review of the literature. J Oral Maxillofacial Surg 68: 1384-1391.
8. Von Wowern N (1982) Closure of oroantral fistula with buccal flap: Rehrmann versus Moczar. Int J Oral Surg 11: 156-165.
9. Abdelhamid AN, Youssef T (2018) Large oroantral fistula repair using combined buccal and palatal flaps: A case series. Egypt J Otolaryngol 34: 48-54.
10. Ogle OE (2002) The management of oronasal fistulas in the cleft palate patient. Oral Maxillofacial Surg Clin N Am 14: 553-562.
11. Borgonovo AE, Berardinelli FV, Favale M, Maiorana C (2012) Surgical options in oroantral fistula treatment. Open Dent J 6: 94-98.
12. Scattarella A, Ballini A, Grassi FR, Carbonara A, Ciccolella F, et al. (2010) Treatment of oroantral fistula with autologous bone graft and application of a non-reabsorbable membrane. Int J Med Sci 7: 267-271.
13. Khandelwal P, Hajira N (2017) Management of oroantral communication and fistula: Various surgical options. World J Plast Surg 6: 3-8.

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Otolaryngology and Neurotology Research(ISSN:2641-6956)
- International Journal of Internal Medicine and Geriatrics (ISSN: 2689-7687)



