599
Views & Citations10
Likes & Shares
External quality assessment (EQA) and Internal
Quality control (IQC) is an alternative tool to cross-checking of blood slides
in the quality control of malaria microscopy. This study was aimed to check EQA
and IQA of malaria microscopy in El Obeid City North Kordofan. A total of 76
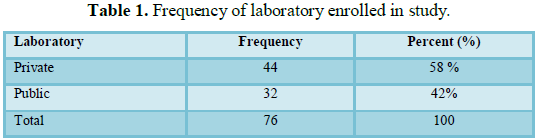
laboratories (55% private and 45% public) were participated in the study.
A well-designed questionnaire plus five blood films
(two negative and three positive films with different parasitemia; (low,
moderate and high) were distributed for each laboratory under study. Two slides
(stained and unstained) blood films and one ml of Geimsa stain were collected
from each laboratory.
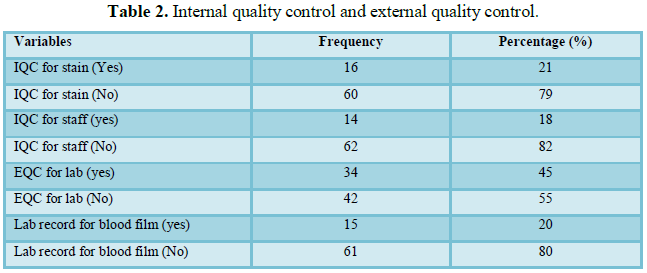
The study revealed that, most of laboratories were
using Geimsa, but the EQA and IQC for both staff and stain were demonstrated
poor performance. Although, only 20% had a record for malaria results, 50% of
laboratories reporting only whether the parasite identified or not. 75% were
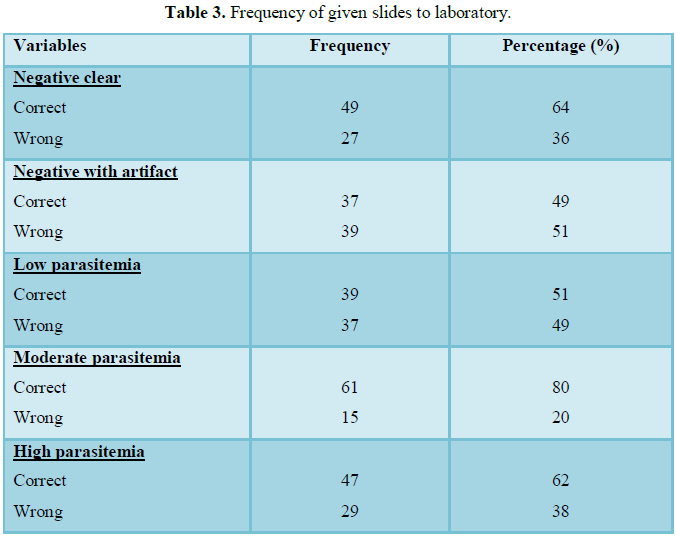
using only thick blood film. The results of the five blood films were; 61% were
correct clear negative, 49% were negative with artifacts, while the three
positive slides were correctly as follows; low (49%), moderate (76%) and (59%)
of high parasite density.
The major errors include; not reporting the density
of malaria low (50%), moderate (31%) and high parasite (13%), but those
reporting wrong were low (24%,) moderate (39%) and high parasite (24%).
The study concludes that, the EQA and IQC of
microscopical examinations for malaria parasite in laboratories in ElObeid were
acceptable, further training courses and effective quality assurance scheme
were needed.
Keywords: El-Obeid,
EQA, IQC, Malaria, Microscope
INTRODUCTION
Malaria is a mosquito borne infectious
disease affecting humans and other animals caused by parasitic protozoan’s
belonging to the genus Plasmodium [1]. Malaria causes symptoms that typically
include fever, vomiting and headache [2]. The disease is most commonly
transmitted by an infected female Anopheles mosquito [3]. The mosquito bite
introduces the parasites from the mosquito’s saliva into person’s blood [4].
The parasites travel to the liver where they mature and reproduce. Four species
of Plasmodium’s can infect and be spread by humans (P. falciparum, P. vivax, P. ovale and P. malariae) [3]. The species P.
knowlesi is rarely causes disease in humans [5]. Most deaths are caused by P. falciparum but the others species
were caused milder form of malaria [6]. Malaria is typically diagnosed by the
microscopic examination of blood using blood films or with antigen based rapid
diagnostic tests [7].
Several medications are available to prevent
malaria in travelers to areas where the disease is common [13,14].
MATERIALS AND
METHODS
This is a cross sectional descriptive study
was conducted during the period of March to August 2017 in El Obeid city, North
Kordofan which is located about 588 km west of Khartoum, longitude 13.11 North
and latitude 30.12 East.
The populations enrolled in this study were
included medical laboratories providing microscopical examination for malaria
in El Obeid. About 76 laboratories (32 public and 44 private).
Each laboratory that offer blood film
examination for malaria in El Obeid were included in this study while those not
carried out malaria microscopical examination were excluded from the study.
ETHICAL
CONSIDERATIONS
The health authorities at the state and
locality levels were informed about the study which was only started after
having their permission and all individuals enrolled in this study were being
asked to participate in the study and an informed consent was obtained.
DATA COLLECTION
TOOLS
A well designed questionnaire were used to
collect general and technical data, and the result of slides that were
distributed as a part of evaluation process as well as 1 ml Giemsa stain were
collected from each laboratory enrolled in the study.
STUDY PROCEDURE
After having consent, the questionnaire was
completed by the interviewer. Then a total of (5) slides were submitted for
reading by the person who routinely perform blood film examination. These
slides included; one slide with no malaria parasite, another slide with no
malaria parasite, but containing stain deposits, and three slides with malaria
parasites; low, moderate and high parasitemia. From each participant
laboratory; one stained and one unstained blood film were selected randomly as
well as getting 1ml Geimsa stain.
DATA ANALYSIS
All data was recorded in standard master
sheets from the questionnaire that was filled by the investigator, and then
were analyzed by the statistical package for social sciences (SPSS) program
version 20.
RESULTS
The
result for blood film with low parasitemia participant were reported true 39
(51%) and wrong were 37 (49%), moderate parasitemia true result were 61 (80%)
and wrong were 15 (20%), and high parasitemia truer were 47 (88%) and false
were 19 (12%) as shown in Table 3.
The major errors include; not reporting the
density of malaria (low 52%, moderate 33% and high parasite 20%), but who
reporting wrong were (low 49%, moderate 20% and high parasite 12%).
DISCUSSION
This study is an attempt to evaluate the
reliability of malaria microscope looking through both variation of result and
associated quality assurance basics (general condition of microscopes,
qualification and experience of technologist). The study assumption is that any
defect in one or more of these basics will consequently affect the reliability
and accuracy of the laboratory results. From the result most of the checked
laboratories were private constitute almost about more than half (personal
contact). Considerable number of them was established 6-15 years ago, about
half are well experienced personnel. Qualification is high and has an academic
certificate; BSc, MSc and even PhD holders). This may be in part due to the
medical laboratory college had 15 years since it was established. About
two-third experienced a basic malaria course, while the majority attended
refresh. Most of laboratories used Geimsa (91%) with the correct concentration
(10 % for 10 min and 3% for 30 min).
The result showed that severe shortage in IQC
for laboratory staff and stain only 14 (18%) for both, on the other side the
majority of them were haven’t EQC (55%) since the duration of EQC are monthly
(33%) quarterly (8%) and (59%) are not. This could be referred to neglecting,
will nestles and weak supervision.
From the result most of the laboratories use
good oil immersion with good condition of microscopes which gives correct true
negative result and false negative result. These can be on line with the study
that done by Merghani et al. [15] in Dongola when using good efficient
microscopes they give low false positive result.
Writing a full report is of great value, but
only 50% laboratories making blood film report with insufficient data this
agree with the study done by Mukadi et al. [16] conducted in the Democratic
Republic of Congo.
Most of laboratories (46%) make only thick
blood (79%) with low quality (14%) and the blood doesn’t give chance for
detection of parasite species and this can affect treatment. The study has
focused on the way in which blood is collected, spread, and dried and if it has
any influence on sensitivity on parasite detection.
The results obtained from blood films
distributed to laboratory revealed that; result of the negative clear true is
about 49 (64%) and false is 27 (36%, blood film with low parasites count true
were 39 (51%) and wrong were 37 (49%) , moderate parasites true result were 61
(80%) and wrong were 15 (20%) and result of blood film with high parasites
count true answer were 47 (88%) and false were 19 (12%), study by Hamdy and
Aljafari (2017) in Khartoum [17] reported (44.3%) those who report density of
parasite true.
CONCLUSION
From the result of the current study, it is
concluded that the most frequent laboratories technicians in the area of the
study were acceptable works but need more IQC as soon as strong EQA.
1. Colwell
DD, Dantas-Torres F, Otranto D (2011) Vector-borne parasitic zoonoses: Emerging
scenarios and new perspectives. Vet Parasitol 182: 14-21.
2. Reisinger
EC, Fritzsche C, Krause R, Krejs GJ (2005) Diarrhea caused by primarily
non-gastrointestinal infections. Nat Clin Pract Gastroenterol Hepatol 2:
216-222.
3. Cox
FE (2010) History of the discovery of the malaria parasites and their vectors.
Parasit Vectors 3: 5.
4. Waitayakul
A, Somsri S, Sattabongkot J, Looareesuwan S, Cui L, et al. (2006) Natural human
humoral response to salivary gland proteins of Anopheles mosquitoes in
Thailand. Acta Trop 98: 66-73.
5. Kantele
A, Jokiranta TS (2011) Review of cases with the emerging fifth human malaria
parasite, Plasmodium knowlesi. Clin
Infect Dis 52: 1356-1362.
6. Baird
JK (2013) Evidence and implications of mortality associated with acute Plasmodium vivax malaria. Clin Microbiol
Rev 26: 36-57.
7. Azikiwe
CC, Ifezulike CC, Siminialayi IM, Amazu LU, Enye JC, et al. (2012) A
comparative laboratory diagnosis of malaria: Microscopy versus rapid diagnostic
test kits. Asian Pac J Trop Biomed 2: 307-310.
8. Tangpukdee
N, Duangdee C, Wilairatana P, Krudsood S (2009) Malaria diagnosis: A brief
review. Korean J Parasitol 47: 93-102.
9. Ndao
M, Bandyayera E, Kokoskin E, Gyorkos TW, Dick MacLean J, et al. (2004)
Comparison of blood smear, antigen detection and nested-PCR methods for
screening refugees from regions where malaria is endemic after a malaria
outbreak in Quebec, Canada. J Clin Microbiol 42: 2694-2700.
10. Karunamoorthi
K (2011) Vector control: A cornerstone in the malaria elimination campaign.
Clin Microbiol Infect 17: 1608-1616.
11. Walker
K, Lynch M (2007) Contributions of Anopheles larval control to malaria
suppression in tropical Africa: Review of achievements and potential. Med Vet
Entomol 21: 2-21.
12. Raghavendra
K, Barik TK, Reddy BP, Sharma P, Dash AP (2011) Malaria vector control: From
past to future. Parasitol Res 108: 757-779.
13. Franco-Paredes
C, Santos-Preciado JI (2006) Problem pathogens: Prevention of malaria in
travellers. Lancet Infect Dis 6: 139-149.
14. Lalloo
DG, Hill DR (2008) Preventing malaria in travellers. BMJ 336: 1362-1366.
15. Merghni
MAEM, Elfaki TEM, Alla ABA, Elsadig AA, Saad MBEA (2016) Evaluation of malaria
diagnosis in Dongola city laboratories, northern state, Sudan. J Eur Acad Res
4: 917-932.
16. Mukadi
P, Gillet P, Lukuka A, Atua B, Kahodi S, et al. (2011) External quality
assessment of malaria microscopy in the Democratic Republic of the Congo. Malar
J 10: 308.
17. Hamdy GAA, Aljafari AS (2017) Capacity of the
clinical laboratories of the private sector at Khartoum state-Sudan for the
parasite-based malaria diagnosis. Ann Trop Med Public Health 10: 211-215.
-
 Table 1
Table 1 -
Table 2
-
Table 3
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Agriculture and Forest Meteorology Research (ISSN:2642-0449)
- Journal of Womens Health and Safety Research (ISSN:2577-1388)
- Journal of Genomic Medicine and Pharmacogenomics (ISSN:2474-4670)
- Proteomics and Bioinformatics (ISSN:2641-7561)
- Journal of Astronomy and Space Research
- Food and Nutrition-Current Research (ISSN:2638-1095)
- Advances in Nanomedicine and Nanotechnology Research (ISSN: 2688-5476)


