771
Views & Citations10
Likes & Shares
Considering the increasing resistance of bacteria to
antibiotics and the presence of antibacterial agents in plants, in this study,
the antimicrobial activity of Tecomella
undulata ethanolic extract on antibiotic resistance Acinetobacter baumannii has been studied.
Materials
and methods: The leaves of Tecomella
undulata were collected from Saravan city and extracted by rotary machine. Acinetobacter bomanii strains were
collected from urine specimens of Imam Khomeini and Ali ibn Abi Talib
Hospitals. Minimum inhibitory concentration and minimum bactericidal
concentration were determined by micro dilution method.
Results: The
results of this study showed that the resistance of the strains was to
amoxiclavanic (10%), ampicillin (20%), gentamicin (0%), ceftazidime (0%) and
nitromicin (0%) antibiotics.
The results of this study showed that the lowest
inhibitory concentration of Tecomella
undulata is 0.62 mg/ml, which inhibits 6 strains in this concentration,
while the highest inhibitory concentration is 5 mg/ml, which inhibited 3
strains in this concentration.
Discussion: By
considering the results, obtained and increasing resistance of bacteria to
chemical antibiotics, it is suggested that bacterial compositions of this plant
can be used to treat bacteria.
Keywords: Tecomella undulata, Antimicrobial
activity, Acinetobacter baumannii
INTRODUCTION
Acinetobacter baumannii is one of the most important pathogens in health
centers that cause many infections including bacteremia, pneumonia, meningitis,
urinary tract infections and ulcers. The ability to survive under various
environmental conditions has made this pathogen one of the most common causes
of infection in health centers [1].
Tecomella
undulata is an Antarctic pink or embroidered pomegranate,
an almost evergreen tree that runs in the southern regions of the country such
as Bushehr, Fars and Hormozgan.
In addition, its
distribution in Afghanistan, West Pakistan and southeastern Arabia has been
recorded. Due to medicinal properties, this plant has been considered as a good
treatment [2]. Flavonoid compounds, phytosterol,
flavonol, fatty acids and terpenoses have been identified in various parts of
the plant [3]. It has anti-inflammatory, antimicrobial and anti-oxidant
activity [3,4].
This plant is useful in
draining urine and enlarging the spleen. The skin of the young shoots of the
plant is used for the treatment of syphilis [5]. The purpose of this study was
to evaluate the antimicrobial activity of the ethanolic extract of Tecomella
undulata on the antibiotic-resistant acintobacter bomanii
in Zabol.
MATERIALS AND
METHODS
In this study 20 isolates of Acintobacter baumanni from infected
patients in Imam Khomeini and Ali ibn Abi Talib Hospitals in Zabol were
investigated.
Laboratory procedures
The clinical specimens
were cultured on the McConky Agar and Blood Agar medium then plates were
incubated at 37°C for 24-24 h. An oxidase test was performed in case of growth
after gram staining and observation of cocci and gram negative diplucoxia. In
the next step, by using biochemical tests, cultured on McConky agar and
incubated at 37°C and 42°C, then citrate and moving test were performed on the of
media containing glucose.
Determination of antibiotic susceptibility
Determination of
susceptibility was done by standard Disc diffusion agar. For testing, bacterial
colonies, 0.5 μM MacFarland suspensions were prepared and well-spread over the
Muller Hinton Agar medium. Then Antibiotic discs were placed at standard
spacing. After 24 h incubation at 37°C, the non-growth diameter for each
antibiotic was measured. The results were recorded for each antibiotic
according to the relevant instructions as sensitive, intermediate and
resistant.
Preparation of ethanolic extract
Tecomella
undulata collected from Saravan city and dried. To prepare the
ethanolic extract, 10 g of dried powder were placed inside half-liter erlenn
containing 100 ml of 96% ethanol (to prepare the ethanolic extract). The
contents of the erlenn were mixed at room temperature for 24 h by shaker
machine (Iran) at 130 rpm and then filtered with Wattman No. 2 paper. Solvent
separation from the extract was performed by a rotary machine
(Heidolph-Germany) with the aid of a vacuum pump (vacuum distillation). The
extracts were weighed and then solved in DMSO solvent. The extract was stored
in a refrigerator until use in antimicrobial experiments at 4°C.
Determination of
susceptibility of bacterial strains to different extracts of pomegranate plant
Determination of susceptibility of bacterial strains
to plant extracts was performed using a dilution method in well. Six wells were
created in a solid culture medium and 100 μl of each well was added to the
nutrient medium of Muller Hinton (MHB). Then, to the first well, 100 ml of
diluted solution of the extracts of plants was added and after mixing 100 μl of
the first well, added to the second well, and this was done until the last
well. From the final well, 100 μl of the medium was extracted and 10 μl of the
microbial suspension containing 107 μg/ml which was equal to 0.5
McFarland added and incubated at 37°C for 24 h. The first pill that was
prevented bacterial growth after placing in the incubator was considered as the
minimum inhibitory concentration. In order to ensure, 10 μl from transparent
wells were transferred to the Muller Hinton Agar medium and after 24 h the
first concentration that could eliminate 99.9% of the bacteria was considered
as the minimum bactericidal concentration.
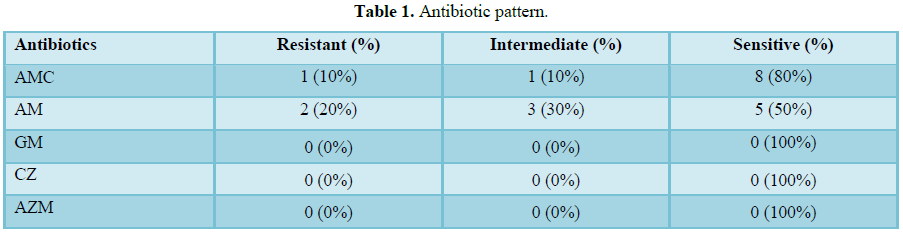
RESULTS
The results of this
study showed that the strains were resistant to amoxicklavanic antibiotics
(10%), ampicillin (20%), gentamicin (0%), ceftazidime (0%) and erythromycin
(0%) (Table 1).
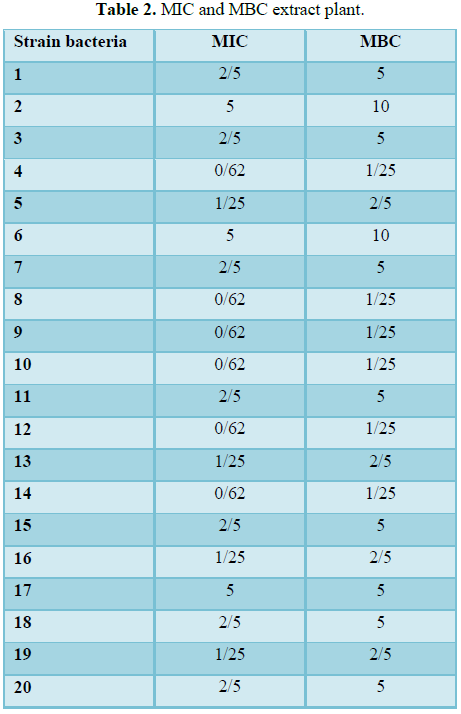
The results of this
study showed that the lowest inhibitory concentration of Tecomella
undulata was 0.62 mg/ml, of which 6 strains were inhibited at
this concentration, while the highest inhibitory concentration was 5 mg/ml
which three strains have been inhibited in this concentration. The highest
bactericidal concentration was 10 mg/ml, which 2 strains were eliminated at
this concentration, while the lowest bactericidal concentration was 1.25 mg/ml (Table 2).
DISCUSSION
The results of this
study showed that the strains were resistant to amoxicklalanic antibiotics
(10%), ampicillin (20%), gentamicin (0%), ceftazidime (0%) and nitromicin (0%)
[6].
The results of this
study showed that the highest resistance was to ceftriaxone, ciprofloxacin and
cefotaxime, which was 99%, observed in Angoti et al. [7], who investigated the
drug resistance of Acinetobacter
baumannii strains in Imam Reza Hospital. The percentage of isolates
resistance to ampicemin, amikacin and ciprofloxacin was 73.3%, 38.3% and 93.3%
in the E-test method, respectively.
The results of Rastu and
Bad [8], who investigated the Acinetobacter
baumannii resistance pattern in Shariati Hospital in Tehran, showed that
the highest sensitivity was to ciprofloxacin (91%), cotrimoxazole (57.5%) and
the highest resistance rate was to ceftriaxone (98.4%).
In the study of Nah et
al. [9], who evaluated the resistance level of Acinetobacter baumannii strains in Tehran city, the results showed
that all isolates of Acinetobacter baumannii
were resistant to ceftizoxime, cefoprazone, ceftazidime, tricarcelin,
clavulanic acid, cefotaxime, aztreonam, Moropenem, cefixim, ceftriaxone,
carbenicillin and ticarcylin, but all isolates were sensitive to cholestin.
The results of Ahmadikiya
et al. [10], who investigated antibiotic resistance of Acinetobacter baumannii in Kerman, showed a resistance rate to
antibiotics such as cefotaxime (100%), ceftazidime (98.9%), cefipime (100%),
aztreonam (98.9%), ampicemin (97.9%), meropenem (97.9%), gentamicin (96.8%),
amikacin (98.9%), ciprofloxacin (97.9%), ciprofloxacin (97.9%) and tetracycline
(90.5%).
In the study of Simhon
et al. [11], Sensitivity to ampicemin was 98.1% in 1990 but reduced to 64.1% in
2000 and the sensitivity to ciprofloxacin decreased from 50.5% to 13.1%. In a
study by Boromand et al. [12] in Tehran, 53.4% of the samples were resistant to
ciprofloxacin and 24.6% resistant to ampicemi.
In the study by Henwood
et al. [13], 46% of the isolates were resistant to ciprofloxacin and 2% of the
samples were resistant to ampicemin.
The results of Zhao
study [14], who investigated the resistant pattern of Acinetobacter baumannii showed a resistance rate to ampicillin
(78.5%), cefazolin (78.5%), imipenem (92.3%), gentamicin (87.7%) and ampicillin
resistance, Ceftazidime (92.3%), aztreonam (92.2%), ciprofloxacin (98.5%) and
tobramycin (81.5%).
The results of Rahbar et
al. [15] study on prevalence of antibiotic resistant showed that resistance to
ceftriaxone (90.9%), piperacillin (90.9%), ceftazidime (84.1%), amikacin (2/85%)
and ciprofloxacin (90.9%).
In the study of
Uwingabiye et al. [16], resistance to antibiotics such as ciprofloxacin,
ceftazidime, piperacillin-tazobactam, imipenin, amikacin, tobramycin,
dabylmezin, rifampin, colistin were 87%, 86%, 79%, 76%, 52%, 43%, 33%, 32% and
1.7%, respectively.
In recent decades, the
research priority has fallen down to make new and effective drugs; this is
despite the fact that the world faces pathogens with drug resistance. Another
concern in this regard is the cost of treating drug-resistant infections due to
the higher cost of new drugs and the long time treatment of
antibiotic-resistant infections than susceptible bacterial infection, which
doubles the importance of finding a new method for treatment [17].
In the study of Abhishek
et al. [18], the minimum inhibitory concentration of methanol extract against B. subtilis, E. fecalis, E. coli, K. pneumonia, M. luteus, P. vulgaris
and P. aeruginosa was equal to
4-0.01-0.1-2.0 mg/ml, respectively. In Thanawala and Jolly [19], Inhibition
diameter of Acetonic extract of Tecomella undulata was compared
to Bacillus subtilis (17 mm) and Staphylococcus
aureus (10 mm), while the inhibitory diameter of alcoholic extract of Tecomella
undulata against the Escherichia
coli was 9 mm.
CONCLUSION
Considering the obtained
results and the increasing resistance of bacteria to chemical antibiotics, it
is suggested that, to conduct more studies on antibacterial compounds of this
plant in treatment of bacterial infections.
1. Amudhan
SM, Sekar U, Arunagiri K, Sekar B (2011) OXA beta-lactamase-mediated carbapenem
resistance in Acinetobacter baumannii.
Indian J Med Microbiol 29: 269-274.
2. Anonymous
(1982) The wealth of India. Raw Materials, Tecoma: CSIR New Delhi 10: 136-139.
3. Jain
M, Kapadia R, Jadeja RN, Thounaojam MC, Devkar RV, et al. (2012) Traditional
uses, phytochemistry and pharmacology of Tecomella
undulate - A review. Asian Pac J Trop Biomed 2: S1918-S1923.
4. Laghari
AQ, Memon S, Nelofar A, Laghari AH (2013) Tecomella
undulata G. Don: A rich source of flavonoids. Ind Crops Prod 43: 213-217.
5. Khatri
A, Garg A, Agrawal SS (2009) Evaluation of hepatoprotective activity of aerial
parts of Tephrosia purpurea L. and
stem bark of Tecomella undulate. J.
Ethnopharmacol 122: 1-5.
6. Chopra
RN, Nayar SL, Chopra IC (1956) Glossary of Indian Medical Plants. 1st
Edn. C.S.I.R: New Delhi 21: 240.
7. Angoti
G, Godarzi H, Besharat M, Hajizadeh M, Zarringhalam Moghaddam M (2014) Evaluation
of antibiotic resistance of clinical Acinetobacter
baumannii isolated of Tabriz Hospital by disk diffusion and MIC methods.
Res Med 38: 106-110.
8. Rastu
A, Bad Y (2009) Frequency of Acinetobacter
baumannii isolated from blood culture in a hospital laboratory Shariati
Tehran. J Paramed Tehran Univ Med Sci 3: 70-75.
9. Nah
SF, Ranjbar R, Ghasemi A, Pakzad A, Zaemi Yazdi, et al. (2006) Evaluation of
drug resistance of Acinetobacter
baumannii and other Acinetobacter species isolated from three hospitals in
Tehran. Sci J Elam Univ Med Sci 3: 14.
10. Ahmadikiya
F, Mosadegh A, Moradi M, Hossieni-Nave H (2017) Antimicrobial resistance
patterns and frequency of extended-spectrum beta-lactamase genes among Acinetobacter baumannii. JBUMS 19:
28-34.
11. Simhon
A, Rahav G, Shazberg G, Block C, Bercovier H, et al. (2001) Acinetobacter baumannii at a
Tertiary-Care Teaching Hospital in Jerusalem. J Clin Microbiol 39: 389-391.
12. Boromand
M, Akyani M, Sheikhvatan R, Hekmat Yazdi S, Saboorian R, et al. (2009)
Evaluation of antimicrobial resistance of Acinetobacter
baumannii to imipenem, ciprofloxacin and ceftazidim using E test. Iran J
Publ Health 2: 130-133.
13. Henwood
C, Gatward T, Warner M, James D, Stockolale M, et al. (2002) Antibiotic
resistance among clinical isolates of Acinetobacter in the UK and in vitro evaluation of Tigecycline
(GAR-936). Antimicrob Chemother 49: 479-487.
14. Zhao
SY, Jiang DY, Xu PC, Zhang YK, Shi HF, et al. (2015) An investigation of
drug-resistant Acinetobacter baumannii infections in a comprehensive
hospital of East China. Ann Clin Microbiol Antimicrob 14: 7.
15. Rahbar
M, Mehrgan H, Aliakbari NH (2010) Prevalence of antibiotic-resistant Acinetobacter baumannii in a 1000-bed
Tertiary Care Hospital in Tehran, Iran. Indian J Pathol Microbiol 53: 290-293.
16. Uwingabiye
J, Frikh M, Lemnouer A, Bssaibis F, Belefquih B, et al. (2016) Acinetobacter
infections prevalence and frequency of the antibiotics resistance: Comparative
study of intensive care units versus other hospital units. Pan Afr Med J 23:
191.
17. Overbye
KM, Barrett JF (2005) Antibiotics: Where did we go wrong? Drug Discov Today 10:
45-52.
18. Abhishek
S, Ujwala P, Shivani K, Meeta B (2013) Evaluation of antibacterial activity of Tecomella undulata leaves crude
extracts. Int Res J Biol Sci 2: 60-62.
19. Thanawala
PR, Jolly CI (1993) Phyarmacognostical phytochemical and antimicrobial studies
on stem bark of Tecomella undulate
seem. Ancient Science of Life 3-4: 414-–419.
-
 Table 1
Table 1 -
Table 2
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Food and Nutrition-Current Research (ISSN:2638-1095)
- Journal of Agriculture and Forest Meteorology Research (ISSN:2642-0449)
- Journal of Womens Health and Safety Research (ISSN:2577-1388)
- Journal of Genomic Medicine and Pharmacogenomics (ISSN:2474-4670)
- Journal of Veterinary and Marine Sciences (ISSN: 2689-7830)
- Proteomics and Bioinformatics (ISSN:2641-7561)
- Advances in Nanomedicine and Nanotechnology Research (ISSN: 2688-5476)


