386
Views & Citations10
Likes & Shares
Information has a relevant role in the prevention of spreading of
HIV/AIDS by widen the knowledge of People Living with HIV/AIDS (PLWHA). The
prospect of information to be provided has to risk practices specific. This
becomes necessary because PLWHA are evidently engaged in series of risk
practices causing new infections among their relative and close associates.
This work explored the level of PLWHA understanding of certain and common risk
practices to identify their information needs.
The study adopted a survey research design which was conducted among
PLWHA attending outpatient departments from five tertiary health institutions
South-West, Nigeria. The study found out a positive correlation between
information needs and risk practices and appropriate recommendations were made.
Keywords: HIV, Information,
Risk practices, PLWHA
INTRODUCTION
Information needs examine and express the psychological state that
first motivates a person to engage in information behaviour. According to
Sokari [2], everybody needs information for variety of purpose ranging from
freedom from bondages associated with ignorance, delusion, false impression,
economic indolence, health problems, communal strife and political
unpredictability. Information needs are connected to obstacles, difficulties
and challenges and an imperative concern is the manner by which those problems
are assumed, defined and originated. Nicholas [3] argues that information needs
emerge out of the aspiration to satisfy one of the indispensable human needs.
Nonetheless, information is not categorized as a principal necessity as the
need for food or security for instance, according to Wilson [4] the need to be
informed might be necessary to meet completely or partially the basic human
needs. People hardly possess the information need itself until when problems are
experienced or people are pressured by certain conditions, then they see a need
for information for the purpose of completely or incompletely addressing such
cases and achieving their ultimate objective. This confirms Belkin and
Vickery’s [5] conclusion, who stated that recognizing a gap in knowledge gives
rise to information needs.
People living with HIV/AIDS (PLWHA) information needs are all-inclusive
and extend to information on medical and social service, medication and correct
usage, level of improvement in their health
and financial empowerment
Risk means interacting with precariousness intentionally. It is
ubiquitous in all areas of life. It is an unpredictable outcome of a deed [7].
Risk involves potential of gaining or losing something of value. Although
everyone is at risk of getting infected with HIV, particular behaviors
constitute risk practices which fan the spread and expansion of this infection.
These majorly include engagement in high risk sexual behaviors, injectable drug
use, blood transfusion and sharing of sharp objects. Others are mother to child
transmissions which often occur by non-screening of mothers for HIV virus
during pregnancy and absence of intervention in time of labor and
breast-feeding. Risk Practices among PLWHA are indicated by evidences of
engagement in activities such as unprotected sex, none or improper condom
usage, multiple sexual partners, consumption of alcohol and other mood altering
substances, stoppage of medication, missing of medical appointments,
indiscriminate sharing of sharps and acquisition of sexually transmitted
disease such as gonorrhea, syphilis among others.
Provision of adequate information empowers PLWHA and alters the notion
of imminent deaths associated with HIV infection if only they keep away from
risk practices. It gives them the mind-set that they are in control of their
situations and not the virus as commonly insinuated. Wealth of information
provides coping and managing strategies on how to positively live with HIV
infection and subsequent development and adoption of risk avoidance plans. Not
only have these information in form of health education assisted HIV positive
individuals and communities to acquire the knowledge and resources essential to
live healthy. It arises whenever individuals assess their knowledge
infrastructures about HIV related risk practices and discover deficits or much
shortfall in required knowledge to deal with the situation such as quality of
life. Moreover, it may come up when PLWHA realise through their internal models
of environment, knowledge, actions, etc. are insufficient to attain the
appropriate goals which may require input from external resources in order to
attain the degrees of certainty required for reasonable action. Outcome of
assessment of knowledge infrastructure may interplay the cognitive perception
leading to the understanding of the real situation about HIV/AIDS related risk
practices. The gaps observed will enable PLWHA to comprehend the real situation
about how risk practices can put their own life at danger of sexually
transmitted infection (STI), exposure to another strains of HIV, among others,
thereby stimulate change towards adoption of risk free and excellent life.
People living with HIV/AIDS (PLWHA) are the main reservoirs of HIV
infection to potential infectors which include their relatives and close
associates. The mode of transmission of this disease is closely related to high
risk sexual behaviors, drug and stimulant consumption, injectable drug use and
sharing of sharp objects which are all categorized as risk practices. PLWHA
attending clinics are counseled regularly through health talks, workshops and
seminars, courses of adherence counseling, warning messages in posters and
leaflets, radio, television programs and through other sources on the dangers
in engaging in any of the risk practices. The information at the disposal of
PLWHA is expected to reduce their risk practices, yet risk practices are still
evidently sustained among them thereby complicating the collaborative responses
of government, international bodies and other stakeholders’ struggles and
determination to control the spread of HIV infection in Nigeria. The study
therefore sought to explore the connection between information needs and risk
practices among PLWHA in South-West, Nigeria.
OBJECTIVE OF THE STUDY
1. Find out information needs among PLWHA in
South-West, Nigeria;
2. Investigate the risk practices among PLWHA
in South-West, Nigeria;
3. Examine the relationship between
information needs and risk practices among PLWHA in South-West, Nigeria.
RESEARCH QUESTIONS
The study attempted to answer
the following questions:
1. What are the major information needs among
PLWHA in South-West, Nigeria?
2. What are the risk practices among PLWHA in
South-West, Nigeria, Nigeria?
HYPOTHESIS
The study was tested under the following research hypothesis at 0.05
level of significance:
1. There is significant relationship between
information needs and risk practices among PLWHA in South-West, Nigeria.
Significance of the study
It is believed that this work would be beneficial to the PLWHA in
ascertaining their information needs. It would also help health information
managers, health librarians and information specialists to design information
functional formation system adapted towards the needs of the PLWHA, through the
understanding of their information needs and preferences.
Methodology
The study adopted the survey research design. The design is
quantitative method of data collection to determine whether significant
relationship occurs between two or more variables. This study attempted to
establish the relationship of information needs on risk practice among PLWHA in
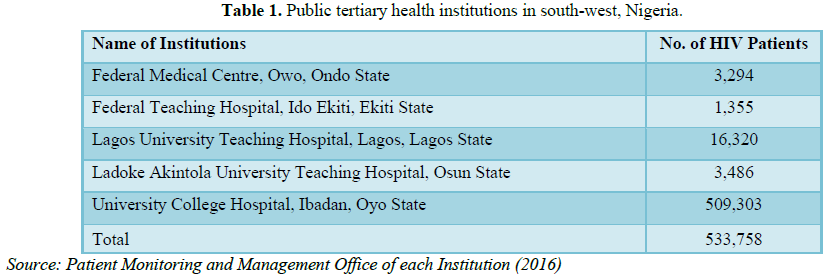
the South-Western Nigeria. According to synthesized data of NACA (2015), the
prevalence rate of HIV in Nigeria was 3.4%. The population of this study
comprises of PLWHA that had ever attended clinics in public tertiary health
institutions in the South-West zone of Nigeria. The total of population of the
HIV/AIDS patients in the tertiary health institutions is 537,234 as shown in Table 1.
To draw sample for this study, an institution was purposively chosen
per state to give equal representation to the all the states in the region. A
pooled standard error of proportion was used to obtain minimum sample size of
103 participants per state using 5% percent margin error as the norm when
dealing with human population [8]. The calculation goes thus:
N2=(Zα + Zβ) 2 × p (1-p)
E2
Where, Zα at 5% of confidence=1.96; Zβ at 80% of power=0.84; P=HIV
national prevalence of 3.4% or 0.034; E at 5% of margin error=0.05
N=(1.96+0.84) 2 * 0.034 *
0.0966
0.052
=7.84 * 0.033
0.05 2
=
0.257
0.0025
=02.99
Pooled standard error of
proportion
Additional 10% was considered for response bias.
Critical Incident technique was used to select the population of the
one hundred and thirteen (113) consenting respondents who were adults from each
of the Four (4) Federal University Teaching Hospitals and Federal Medical
Centres their clinics. The total sampling size was five hundred and sixty five
(565) respondents. Questionnaire was distributed during the clinic days with
the highest attendances in out-patient clinics of the selected hospitals. Only
five hundred and ten (510) copies which represent 90% were analysed as other
copies were found not to be good enough for analyses.
FINDINGS AND DISCUSSION
Presentation of results
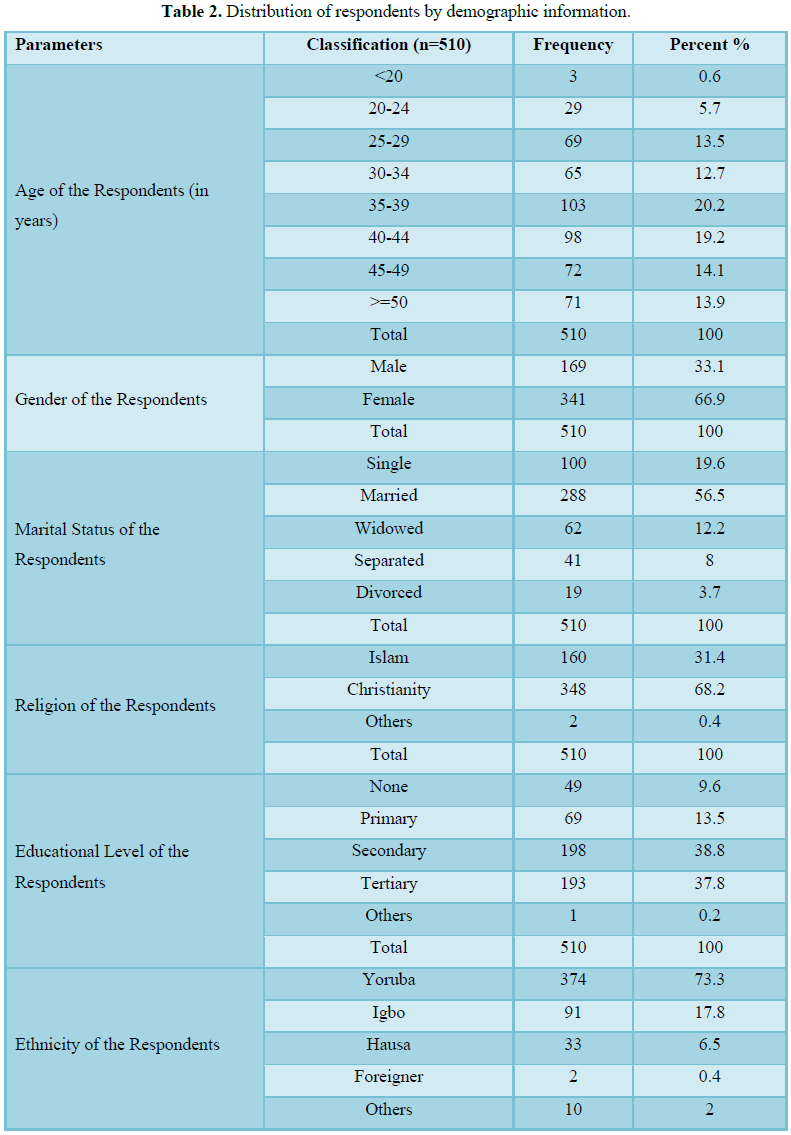
Results are shown in Table 2.
Table 2 shows that most of the respondents were
between the ages 35-36 (20.2%), followed by people of ages 40-44 years (19.2%),
then people of ages 50 and above (13.9%). This was followed by the respondents
of ages 25-29 years (13.5%), then people of ages 45-49 years (14.1%), then ages
30-34 years (12.7%), 20-24 years (5.7%). The least age group among the
respondents was less than 20 years (0.6%). This results implies that majority
of the respondents were youth and young adults.
Moreover, analysis of the participants in this study by gender
indicated that 33.1% were males while 66.9% were females. This implies that
majority of the respondents were females. Analysis of respondents by marital
status revealed that most of the respondents were married (56.5%), 19.6% were
single, 12.2% were widowed, 8.0% were separated, while minority of them were
divorcees 3.7%. This suggested that majority of the respondents had marital
commitment or a lot of them were couples.
In addition to these, Table
1 denotes that 68.2% of the respondents
were Christians, 31.4% were Muslims while 0.4% of the respondents practices
other religions. Furthermore, it can be deduced from Table 1 that only 9.6% of the respondents had no formal education.
Most of the respondent 38.8% had secondary education, while 37.8% had tertiary
education, 13.5% had primary education, while 0.2% claimed to have other level
of education. This implies that majority of the respondents were educated.
Analysis by the ethnicity of the respondents depicts Yoruba ethnic group to be the majority 73.3%, followed by
Igbos 17.8%, Hausas 6.5% and other Nigerians 2.0%. Foreigners constituted
minority 0.4%. This indicates that all major ethnic groups in the country
participated in the study, though the Yoruba ethnic group formed the significant
part, possibly because the study is centred on South-West geopolitical zone.
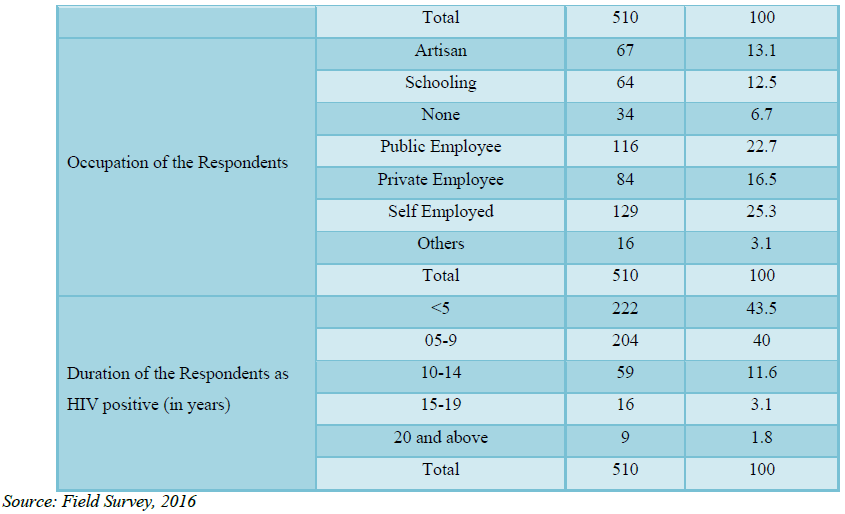
The bulk of the respondents (25.3%) were self-employed, 22.7% were public
employees, 16.5% were private employees, 13.15 were artisans, students
constituted 12.5% each, 3.1% do other works. 6.7% of the respondents had no
work. This means good percentage of them had means of livelihood.
Analysis by duration of the respondents as HIV positive (in years)
shows that 43.5% of the respondents have been living with the infection in less
than five years ago, 40.0% knew their HIV positive status between 5-9 years
ago, 11.6% knew their status between 10-14 years ago while 3.1% knew they had
the virus 15-19 years ago. 1.6% became aware of HIV status in at least 20 years
ago. This implies that all the respondents knew they were HIV positive.
Research question one: What are
the major information needs among people living with HIV/AIDS in south-west
Nigeria?
Table 3 shows the major information needs among
PLWHA in south-west Nigeria. The percentages of strongly agree and agree were
summed up to form percentage of agreement. Considering the result obtained, the
most important information needed by PLWHA was information about status
disclosure as indicated by 47.8% of the respondents, followed by information on
spiritually and HIV medication (20.8%), then, clarification of false beliefs
and misconceptions about HIV/AIDS 11.6%. Additionally, PLWHA needed information
about risk factors aiding HIV/AIDS (5.9%), gonorrhea and other sexually transmitted
diseases (5.7%), then information on dangers in drugs and alcohol consumption
(4.5%) followed by information about HIV/AIDS risk practices avoidance plan
(4.5%), infectivity (3.5%) and information about the importance of social
support in HIV/AIDS management (3.2%). Information needs on the use of
recommended medication and information on risk practices avoidance were of the
2.6% each.
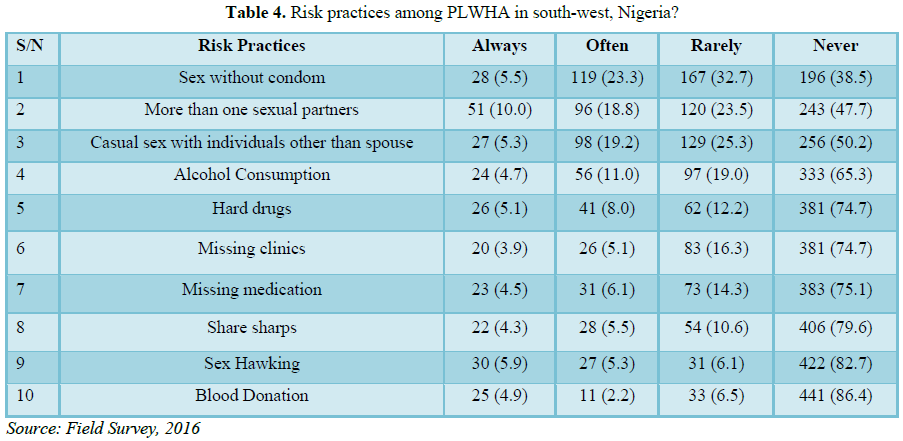
Research question two: What are
the risk practices among PLWHA in south-west, Nigeria?
PLWHA were still evidently engaging in virtually all the HIV/AIDS
related risk practices stated in the instrument according to Table 4. Percentage of risk practices
of the respondents per item was calculated by adding the fractions of always,
often and rarely responses together. The table was arranged in ordered form,
from highest risk practices to the least one. Sex without condom was the most
common (61.5%) risk practices engaged in by PLWHA, followed by multiple sexual
partners (52.3), the casual sex with individual beside the spouse (49.8%),
followed by alcohol consumption (34.7%), then missing of their medical
appointment and engagement in consumption of hard drugs recorded the same
percentage 25.3, then, non-adherent to medication (24.9%), while 20.4% still
share sharp objects. 17.3% hawked sex while 13.6% donated blood.
Risk practices among PLWHA
PLWHA were still evidently engaging in virtually all the HIV/AIDS
related risk practices stated in the instrument. Sex related risk practices
were found to be most common among PLWHA. Sex without condom was the most
common, followed by multiple sexual partners, the casual sex with individual
beside the spouse. This is in line with the opinion of Timothy and Palmer [9]
which stated that risk practices among PLWHA is associated with mode of
transmission which include engaging multiple sexual partners, unprotected
sexual intercourse, sharing of needles and syringes by Injectable Drug Users
among others. The duo also opines that PLWHA spreading of HIV infections by
engaging high-risk sexual practices, hard drug consumption among others.
Kalichman [10] also established that HIV transmission risk practices have
become prevalent among PLWHA that one in three members of this group still
engage in the practice. Consumption of alcohol and hard drugs were also found
to be very common. This result corroborates with the outcomes of Dangerfield et
al. [11] in their research in Kuala, Malaysia report that HIV/AIDS is of high
prevalence among drug and alcohol users. Moreover, this is line with the
argument of Parry [12], Parker et al. [13] and Kotchick et al. [14] that sexual
risk practice as an activity that is performed under the influence of mood
altering items like alcohol. The study also revealed that PLWHA were still in
the habit of non-adherent to medication prescription and missing of medical
appointment. This according to Yaya et al. [15] forms part of challenges of
PLWHA use of information along with low education level, non-adherence to ART,
alcohol consumption before sex, the duration on ART. Sex hawking and sharing of
sharp objects were performed on the same scale each. The least perpetuated risk
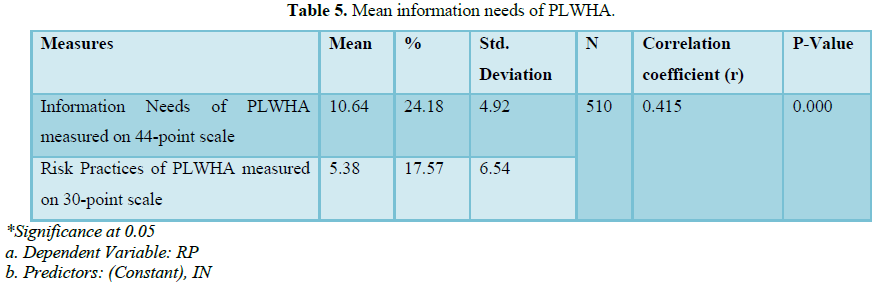
practice according to Table 5 was
blood donation.
Analysis of Table 5 reveals
that the mean information needs of PLWHA was 10.64 and SD=4.81 and that of risk
practices was 5.27 and SD=6.38. Other information derived from the table shows
that a positive and significant relationship between information needs and risk
practices of PLWHA (r=0.415, p<0.05). Therefore, the null hypothesis is
rejected and the research hypothesis is accepted and restated that there is a
significant relationship between information needs and risk practices among
people living with HIV/AIDS [16,17].
Information needs of PLWHA found to have positive significant
relationship with risk practices among PLWHA both individually and mutually.
The positive relationship between information needs and risk practices implies
that the more the information needs the more the likelihood of engaging in risk
practices by PLWHA and vice versa [18,19].
SUMMARY
The major findings of the study include:
1. The major risk practices PLWHA engaged in
were all sexually related and include sex without condom, multiple sexual partners,
sex hawking and casual sex with individual beside the spouse. These were
followed by consumption of alcohol and hard drugs, non-adherent to medication
prescription and missing of medical appointment.
2. PLWHA needed information critically as
regards issues of infectivity, false beliefs and misconception, medication
adherence, status disclosure and transmission risk factors, HIV and
spirituality, risk avoidance and social support in order to reduce their risk
practices. The information needs of PLWHA was found to be low, hence the low
percentage of risk practices. The more the information needs the more the risk
practices.
RECOMMENDATIONS
1. PLWHA should be well educated on the
importance of safe sex practices and other preventive measures such as faithfulness,
abstinence where possible and proper use of condom to reduce transmission of
HIV through sexual intercourse. In connection to these, the government should
as a matter of policy, introduce sex education in school curriculum from
secondary school to other higher institutions of learning in the country. In
addition to these health agencies such as the National Action Committee on AIDS
(NACA) in partnership with their international counterparts, such as USAID,
UNAIDS, GHAIN need to incorporate behavioral change communication with emphasis
on safe sex with biomedical and structural approaches to the management of HIV
infection.
2. In an effort to address the issue of risk
practices reduction among PLWHA, it is important that information specialists
team up with other stakeholders to repackage information on infectivity, false
beliefs, risk avoidance strategies, medication adherence, status disclosure and
transmission risk factors, HIV and spirituality and social support into
animation, visualization and drama series to address their HIV/AIDS risk
practices information needs. This will aid their better understanding and
invariably improve their information behavior. It would however be advisable
that such information is made available to them through electronic and print
sources.
1. Losce RM (1990) Society development and
libraries. Center for External Studies: University of Ibadan.
2. Sokari U (2006) The role of library and
information management in promotion of information Literacy in the 21st century
in Nigeria. Int J Res Educ 3: 125.
3. Nicholas D (2000) Assessing information
needs: Tools, techniques and concepts for the internet age. 2nd Edn.
London: Aslib.
4. Wilson TD (2000) Models in information
behavior research. J Documentation 55: 249-270.
5. Belkin NJ, Vickery A (1985) Interaction in
information systems: A review of research from document retrieval to
knowledge-based systems. British Library, Library and Information Research
Report 35: 246
6. Opeyemi A (2016) Meaning in life and
information behavior of people living with HIV/AIDS in Oyo state, Nigeria. J
HIV AIDS 2.
7. Smith DM, Richman DD, Little SJ (2015) HIV
super infection. J Infect Dis 192: 438-444.
8. Saunders M, Lewis P, Thornhill A (2009)
Research methods for business students. 5th Edn.
9. Hogan TP, Palmer CL (2005) Information
preferences and practices among people living with HIV/AIDS: Results from a
nationwide survey. J Med Libr Assoc 93: 431-439.
10. Kalichman SC (2000) HIV transmission risk
behaviors of men and women living with HIV-AIDS: Prevalence, predictors and
emerging clinical interventions. Clin Psychol Sci Pract 7: 32-47.
11. Dangerfield DK, Gravitt P, Rompalo AM, Yap I,
Tai R, et al. (2015) Awareness and utilisation of HIV services of an AIDS
community based organisation in Kuala Lumpur, Malaysia. Int J STD AIDS 26:
20-26.
12. Parry C (2002) South Africa health review,
alcohol and other drug use. Med Res Council 23: 441-454.
13. Parker W, Makhubele B, Ntabalati P, Connolly
C (2007) Concurrent Sexual partnerships among young adults in South Africa:
Challenges for HIV prevention communication. Pretoria: CADRE.
14. Kotchick BA, Shaffer A, Forehand R, Miller KS
(2011) Adolescent sexual risk behavior: A multi-system perspective. Clin
Psychol Rev 21: 493-519.
15. Yaya I, Saka B, Landoh DE, Patchali PM,
Makawa M, et al. (2014) Sexual risk behavior among people living with HIV and
AIDS on antiretroviral therapy at the regional hospital of Sokodé, Togo. BMC
Public Health 14: 636.
16. Adebayo T (2017) Information behavior and
risk practices among people living with HIV/AIDS in south-western, Nigeria. A
Thesis submitted to the Department of Information Resources Management, Babcock
University for the award of Doctor of Philosophy (PhD) in Health Information
Management.
17. Ape R (2012) Meeting health information needs
of people with HIV and AIDS through Public Library Services in Benue state. A
Thesis Submitted to the Department of Library and Information Science,
University Of Nigeria Nsukka for the award of Doctor of Philosophy (PhD) in
Library and Information Science.
18. International Treatment Preparedness
Coalition (ITPC) (2005) Missing the target: A report on HIV/AIDS treatment
access from the frontlines. Retrieved from: http://www.nigeria-aids.org/documents/ITPC_TreatmentReportFinal.pdf
19. Simbayi LC, Kalichman SC, Strebel A, Cloete
A, Henda N, et al. (2007) Disclosure of HIV status to sex partners and sexual
risk behaviors among HIV-positive men and women, Cape Town, South Africa. Sex
Transm Infect 83: 29-34.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Dermatology Clinics and Research (ISSN:2380-5609)
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- Journal of Spine Diseases
- Journal of Alcoholism Clinical Research
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)


