947
Views & Citations10
Likes & Shares
Background: Pre-clinical and clinical data suggest that transplantation of autologous bone marrow stem cells may contribute to myocardial repair. Intracoronary autologous bone marrow mononuclear cell (BM-MNCs) transplantation in patients with severe LV dysfunction and diffused coronary is safe and improves functional outcome.
Methods and materials: Five patients with diffused coronary artery disease and severe LV dysfunction (20-70 years of age) with Left Ventricular Ejection Fraction (LVEF)<30% were included in this study. Mean volume of BM-MNCs (45 ml) infused with dose of mean 0.34% CD34+ cells. Patients were followed-up with catheterization profile and 16 segment echo for 1, 3 and 6 months.
Results and Conclusion: LVEF was significantly increased from 25% to 40% in two of the patients who received approximate dose of 0.4% of CD34+ cells and mean viability of 98%. No adverse events observed during the study period. Patients were absent for follow-up investigations, however two patients were finally traced after ten years with improved quality of life. This study demonstrates that intracoronary infusion of autologous BM-MNCs can be performed with relative safety without inducing new life threatening ventricular tachyarrhythmia
Keywords: Dilated cardiomyopathy, Autologous stem cells, Mononuclear cells, Intracoronary
Abbreviations: AMI: Acute Myocardial Ischemia; APTT: Activated Prothrombin Time; BM: Bone Marrow; BM-MNCS: Bone Marrow Mono Nuclear Cells; DCM: Dilated Cardiomyopathy; ECG: Electro Cardiogram; EF: Ejection Fraction; IEC: Institutional Ethics Committee; LFT: Liver Function Tests; LV: Left Ventricle; LVEF: Left Ventricular Ejection Fraction; NYHA: New York Heart Association; PT: Prothrombin Time; RFT: Renal Function Tests
INTRODUCTION
Dilated (congestive) cardiomyopathy is a group of heart muscle disorders in which the ventricles enlarge but are not able to pump enough blood for the body’s needs, resulting in heart failure. Dilated cardiomyopathy can develop at any age but is more common among people aged 20 to 60 years. About 10% of people who develop dilated cardiomyopathy are older than 65. The disorder occurs in about 3 times as many men as women and 3 times as many blacks as whites. About 5 to 8 of every 100,000 people develop the disorder each year.
Prognosis and treatment
About 70% of people with dilated cardiomyopathy die within 5 years of when their symptoms begin, and the prognosis worsens as the heart walls become thinner and the heart functions less well. Abnormal heart rhythms also indicate a worse prognosis. Overall, men survive only half as long as women and blacks survive half as long as whites. About 50% of deaths are sudden, probably resulting from an abnormal heart rhythm.
About 20-40% of patients have familial forms of the disease, with mutations of genes encoding cytoskeletal, contractile, or other proteins present in myocardial cells [1]. Although the disease is more common in African-Americans than in whites [2] it may occur in any patient population.
The progression of heart failure is associated with left ventricular remodeling, which manifests as gradual increases in left ventricular end-diastolic and end-systolic volumes, wall thinning and a change in chamber geometry to a more spherical, less elongated shape. This process is usually associated with a continuous decline in ejection fraction. Conventional interventions, such as coronary artery bypass graft (CABG) or percutaneous coronary intervention (PCI), are only able to restore heart function to a minor degree, with an improvement in the left ventricular ejection fraction (LVEF) of only approximately 3-4% [3]. Although interventional and conventional drug therapy may delay ventricular remodeling, there is no basic therapeutic regime available for preventing or even reversing this process.
Stem cell therapy has emerged as a promising strategy for the treatment of dead myocardium, directly or indirectly, and seems to offer functional benefits to patients. The Cellular transplantation to improve myocardial function and perfusion has been proven in animal models [4,5] and human pilot studies [6-9]. It has been demonstrated that administration of bone marrow stem cells leads to improved perfusion and left ventricular function.
The present study evaluated the safety, feasibility and efficacy of intracoronary administration of bone marrow mononuclear cells in patients with dilated cardiomyopathy with diffuse coronary artery disease.
METHODS
Patient population
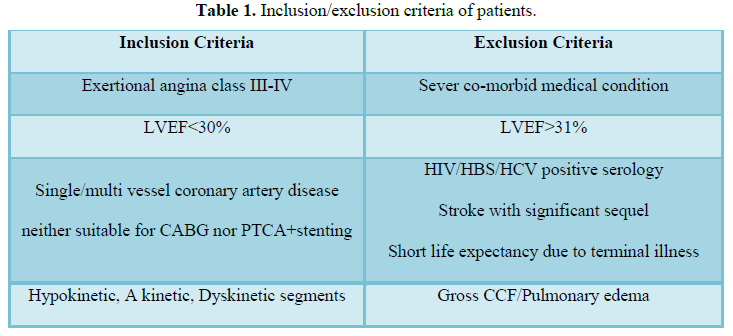
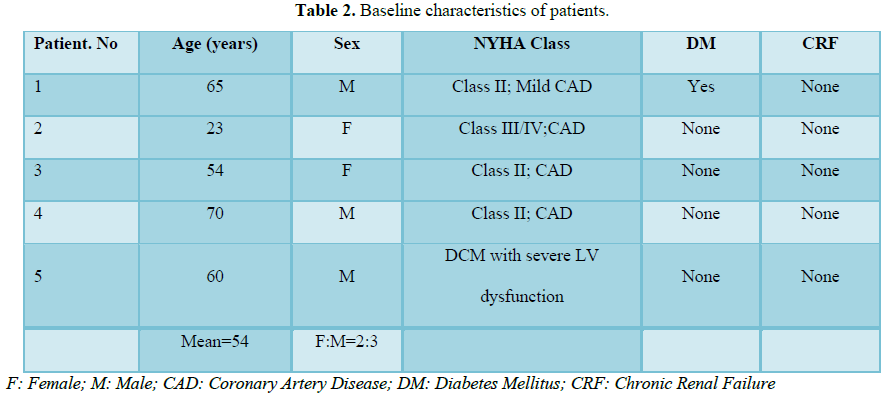
This study has been approved by Institutional Ethics Committee (Dated 10-1-2005; IEC-Global Hospitals, Hyderabad, India). Five patients with a history of dilated cardiomyopathy with severe LV systolic dysfunction with EF<30% falling under New York Heart Association (NYHA) Class II or III were included. Inclusion/Exclusion criteria; pre and post stem cell transplant investigations are listed in the following tables (Tables 1-5).
Bone marrow harvest and cell isolation
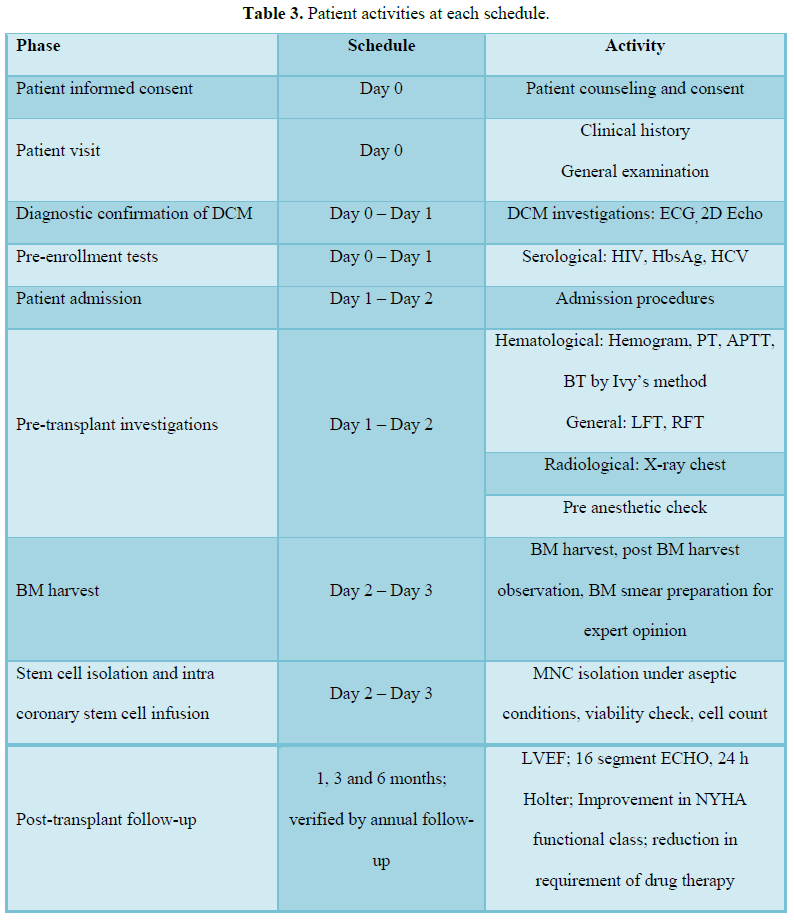
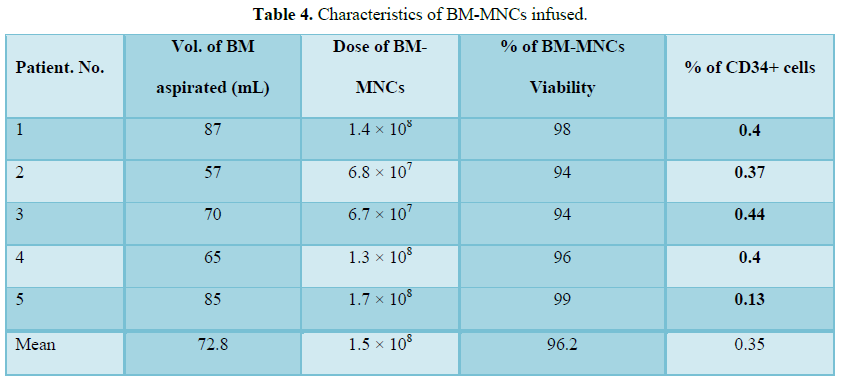
High risk informed consent was obtained from the patient or his/her relatives. Bone marrow was harvested from the posterior iliac crest under deep sedation following standard aspiration protocol on the day of cardiac catheterization. Mononuclear cells were isolated on Ficol-gradient (Sigma). Three washing steps were performed and cells were re-suspended in normal saline for use. All BM manipulation procedures were done under cGMP conditions. Viability was tested by Trypan blue exclusion method (Sigma) and showed viability more than 90% of cells for each transplant. Characteristics of MNCs infused shown in the following tables. Histological evaluation of BM smear preparation revealed normal tissue in all patients. BM-MNCs were kept at room temperature until infusion.
Intracoronary infusion of BM-MNCs
BM-MNCs were infused into the infarct related artery at the site of the previous occlusion. BM-MNCs were suspended in 45 ml of normal saline. 30 ml was injected in the left coronary artery and 15 ml in the right coronary artery slowly through right radial approach. Time taken for left coronary infusion was 10-12 min while of right coronary infusion of 5-6 min. approximately 10cc infusion was administered at one bolus. Patient was discharged from the hospital after 72 h. post procedure.
Outcome measures
Primary end point: Safety and feasibility of the procedure was considered as primary end point on the present study. Any adverse event, concomitant medications, hospitalization and deaths within 6 months of post stem cell infusion were evaluated for safety.
Secondary end points: Improvement in LVEF was considered as efficacy measure. Any signs of new arrhythmias were recorded.
RESULTS AND DISCUSSION
The baseline characteristics of five patients are given in Tables 2 and 4. Intracoronary infusion of BM-MNCs was performed without any acute or long term side effect. No arrhythmatic effects were detected in Holter monitoring during follow-up. There was no episode of ventricular tachycardia observed by Holter monitoring. Remarkable improvement in Echo parameters was observed in three patients who received approximately 0.4% of CD34+ cells with viability of 98%. Significant improvement in LVEF from 25% to 45% was observed. Patients who received less viable cells shown comparatively less LVEF. The improvement in LVEF suggests that intracoronary infusion of autologous BM-MNCs to patients with severe DCM can potentially lead to improved clinical symptoms.
Preliminary studies with lower primate animal models have shown that stem cells can be induced to differentiate onto cardiomyocytes ex vivo [10,11] however similar differentiation was not consistently shown in vivo [12]. A number of clinical trials have proven the safety of stem cell therapy. Bone marrow-derived stem cells (BMCs) infusion represents the greatest number of clinical studies for myocardial ischemia [13]. Single intracoronary transfer of unfractionated BMMNCs in BOOST trial with acute AMI provided only short-term benefits lasted no more than 6 months [14]. In the ASTAMI trial follow-up (24 h to 3 years), there was no effect on global LV function after intracoronary injection of autologous BMMNCs [15-17]. The BMMNCs treated patients (191 patients) in STAR-heart trial with an LVEF of 35% exhibited a statistically significant improvement in LV performance compared suggests that BMMNC therapy can affect mortality in patients with chronic heart failure [18].
Promising results in human clinical trials have been obtained by administering bone marrow stem cells to the area of infarction after revascularization of acute myocardial infarction [19]. TOPCARE-AMI study demonstrated a significant increase in global LVEF and significant decrease in infarct size. Transplanted marrow stromal cells into the rat model of dilated cardiomyopathy improved cardiac function by inhibiting myocardial fibrosis [20]. Expansion of bone marrow-derived MSCs for therapy require at least 7 days compared with unfractionated BMMNCs while the endogenous conditions from each patient may be varied.
In our study we have infused autologous mononuclear cells through both coronaries. The mononuclear cell fraction of bone marrow contains a cocktail of hemangioblasts, endothelial progenitor cells and mesodermal progenitor cells. CD34 is one of the markers for Hemopoietic stem cells (HSCs) that possess kinase insert domain receptor (KDR) and are believed to be able to derive all blood lineages and possibly trans differentiate into cardiomyocytes [21].
It is now evident that secretion of specific growth factors from transplanted stem cells may activate angiogenic, anti-apoptotic and anti-fibrotic paracrine patterning within the recipient heart, playing a major role in tissue repair [22]. Stem cells infused in systemic circulation would require number of circulatory passages to enable the administered stem cells to home at the infarct area. Hence supplying a large bolus of stem cells at the site of infarct area would facilitate homing of more number of stem cells. Moreover the microenvironment and paracrine effect of resident cardiac stem cells also facilitate homing of administered stem cells leading to improved clinical outcome. Stem cell from peripheral blood and cord blood are also being used in exploring clinical trials of cardiomyopathy. The results of the present study are in agreement previous studies using similar stem cells and method of administration [23] and demonstrate that procedure can be performed with relative safety and without inducing new life threatening ventricular tachyarrhythmia.
LIMITATIONS OF THE STUDY
This is a preliminary study designed primarily for evaluation of safety and feasibility of the procedure. CD34+ cell population in the BM-MNCs was not quantified before the time of infusion due to non-availability of FACS caliber that time. Cryo-preserved samples were evaluated for CD34+ cell population after the availability of FACS caliber. Furthermore larger randomized studies are warranted for evaluation. Functional assessments in terms of myocardial viability following stem cell administration are warranted.
CONCLUSION
In patients with dilated cardiomyopathy and diffused coronary artery disease with severe LV dysfunction, the intracoronary infusion of autologous bone marrow mononuclear cells appears to be safe, leading to significant improvement in left ventricular ejection fraction.
ACKNOWLEDGEMENT
Author Dr. G Kavita Marita (Stem cell Physiology), Dr. PLN Kapardhi (Interventional Cardiologist) and Dr. Shailesh R Singhi (Haemato-oncologist) worked as a team in Global Hospitals (2006), Hyderabad where this study was conducted.
1. Ross J Jr (2002) Dilated cardiomyopathy: Concepts derived from gene deficient and transgenic animal models. Circ J 66: 219-224.
2. Coughlin SS, Labenberg JR, Tefft MC (1993) Black-white differences in idiopathic dilated cardiomyopathy: The Washington DC Dilated Cardiomyopathy Study. Epidemiol 4: 165-172.
3. Abbate A, Biondi-Zoccai GGL, Appleton DL, Erne P, Schoenenberger AW, et al. (2008) Survival and cardiac remodeling benefits in patients undergoing late percutaneous coronary intervention of the infarct-related artery: Evidence from a meta-analysis of randomized controlled trials. J Am Coll Cardiol 51: 956-964.
4. Tomita S, Li RK, Weisel RD, Mickle DA, Kim EJ, et al. (1999) Autologous transplantation of bone marrow cells improves damaged heart function. Circulation 100: II247-II256.
5. Jackson KA, Majka SM, Wang H, Pocius J, Hartley CJ, et al. (2001) Regeneration of ischemic cardiac muscle and vascular endothelium by adult stem cells. J Clin Invest 107: 1395-1402.
6. Strauer BE, Brehm M, Zeus T, Köstering M, Hernandez A, et al. (2002) Repair of infarcted myocardium by autologous intracoronary mononuclear bone marrow cell transplantation in humans. Circulation 106: 1913-1918.
7. Assmus B, Schächinger V, Teupe C, Britten M, Lehmann R, et al. (2002) Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction (TOPCARE-AMI). Circulation 106: 3009-3017.
8. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt P, et al. (2004) Intracoronary autologous bone-marrow cell transfer after myocardial infarction: The BOOST randomised controlled clinical trial. Lancet 364: 141-148.
9. Jyotsna M, Vemuganti GK, Reddy P, Chandra KS (2006) Autologous bone marrow-derived progenitor cell myocardial delivery for recent myocardial infarction patients following early angioplasty: Results from a pilot study. Cardiovasc Revasc Med 7: 217-221.
10. Liechty KW, MacKenzie TC, Shaaban AF, Radu A, Moseley AM, et al. (2000) Human mesenchymal stem cells engraft and demonstrate site-specific differentiation after in utero transplantation in sheep. Nat Med 6: 1282-1286.
11. Kehat I, Kenyagin-Karsenti D, Snir M, Segev H, Amit M, et al. (2001) Human embryonic stem cells can differentiate into myocytes with structural and functional properties of cardiomyocytes. J Clin Invest 108: 407-414.
12. Balsam LB, Wagers AJ, Christensen JL, Kofidis T, Weissman IL, et al. (2004) Hematopoietic stem cells adopt mature hematopoietic fates in ischemic myocardium. Nature 428: 668-673
13. Stamm C, Westphal B, Kleine HD, Petzsch M, Kittner C, et al. (2003) Autologous bone-marrow stem-cell transplantation for myocardial regeneration. Lancet 361: 45-46.
14. Meyer GP, Wollert KC, Lotz J, et al. (2006) Intracoronary bone marrow cell transfer after myocardial infarction: Eighteen months’ follow-up data from the randomized, controlled BOOST (BOne marrOw transfer to enhance ST-elevation infarct regeneration) trial. Circulation 113: 1287-1294.
15. Lunde K, Solheim S, Aakhus S, et al. (2006) Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. New Eng J Med 355: 1199-1209.
16. Janssens S, Dubois C, Bogaert J, et al. (2006) Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevation myocardial infarction: Double-blind, randomized controlled trial. Lancet 367: 113-121.
17. Beitnes JO, Hopp E, Lunde K, et al. (2009) Long-term results after intracoronary injection of autologous mononuclear bone marrow cells in acute myocardial infarction: the ASTAMI randomised, controlled study. Heart 95: 1983-1989.
18. Strauer BE, Yousef M, Schannwell CM (2010) The acute and long-term effects of intracoronary Stem cell transplantation in 191 patients with chronic heart failure: The STAR-heart study. Eur J Heart Failure 12: 721-729.
19. Nagaya N, Kangawa K, Itoh T, Iwase T, Murakami S, et al. (2005) Transplantation of mesenchymal stem cells improves cardiac function in a rat model of dilated cardiomyopathy. Circulation 112: 1128-1135.
20. Ventura C, Cavallini C, Bianchi F, Cantoni S (2008) Stem cells and cardiovascular repair: A role for natural and synthetic molecules harboring differentiating and paracrine logics. Cardiovasc Hematol Agents Med Chem.
21. Crosby JR, Kaminski WE, Schatteman G, et al. (2000) Endothelial cells of hematopoietic origin make a significant contribution to adult blood vessel formation. Circulation Res 87: 728-730.
22. Kuethe F, Richartz BM, Kasper C, Sayer HG, Hoeffken K, et al. (2005) Autologous intracoronary mononuclear bone marrow cell transplantation in chronic ischemic cardiomyopathy in humans. Int J Cardiol 100: 485-491
23. Blatt A, Cotter G, Leitman M, Krakover R, Kaluski E, et al. (2005) Intracoronary administration of autologous bone marrow mononuclear cells after induction of short ischemia is safe and may improve hibernation and ischemia in patients with ischemic cardiomyopathy. Am Heart J 150: 986.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- International Journal of AIDS (ISSN: 2644-3023)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Dermatology Clinics and Research (ISSN:2380-5609)


