1091
Views & Citations91
Likes & Shares
Introduction: Non-melanoma
skin cancers (NMSC) are the most common skin cancers in Australia. There are
very few studies which examine the epidemiology of residual and recurrent
non-melanoma skin cancers.
Methodology: Medicare
Australia (MA) billing data pertaining to the treatment of residual and
recurrent NMSC were extracted. Data were
subdivided into three different groups: primary treatment, residual treatment
and recurrent treatments. Each sub-group
was then examined after stratification for state, age and gender. The size of recurrent NMSC was also examined.
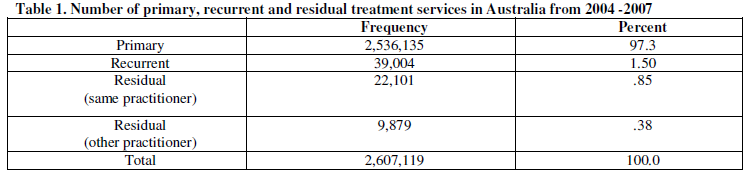
Results: There were
2,536,135 services for the treatment of NMSC, with only 2.73% accounting for
the treatment of residual or recurrent treatments. The proportion of NMSC
treated for recurrence was 1.53%. The proportion of NMSC requiring residual
treatment was 1.26%. Over 71% of NMSCs
treated for recurrence were initially treated by serial cautery and curettage,
radiotherapy or cryotherapy. Approximately 11,594 of original NMSC lesions
requiring a second treatment for residual occurrence were under 10mm,
representing over one half of the residual NMSC billed.
Discussion: In brief,
this study examines the proportion of residual and recurrent cases being billed
to MA. This is the first study which examines rates throughout Australia. While
most studies examine recurrence rates after surgical excision, this study also
takes into account treatment of recurrences using ablative techniques.
INTRODUCTION
Non-melanoma skin cancers (NMSC) are the most commonly occurring cancer
in Australia [1]. It is estimated that they cost the Australian Government $511
million in 2010 alone [2]. Incidence and
prevalence rates of NMSC have been studied extensively over the last 50 years
[1]. In contrast, there are a limited number of studies, which have
investigated the demographics associated with residual and recurrent NMSC,
particularly in the whole of Australia.
Studies in private practices or specialist tertiary centres in
Australia have demonstrated that residual NMSC can occur in anywhere between
0.7% (3) to 12% [4]. Figures for recurrence also vary from 0.7% [3] in a
private practice in Queensland to 8.0% [5] in an Australia-wide study examining
lesions treated with Mohs surgery.
Around the world, recurrence rates have been found to be in the order
of 3.3% to 5% [6-9]. A study by Sussman et al. of 723 BCCs conducted in
Middlemore, New Zealand demonstrated that 11% of primary excisions had residual
tumour cells [10]. By contrast, another study in New Zealand conducted in 1997
examining 61 lesions, found that the rate of residual tumour cells was 31%
[11]. This study however, focuses on
lesions that were excised by General Practitioners (GPs) who where possibly
less experienced than the specialists used in the study by Sussman et al. [10].
The overall rate of incomplete excisions for GPs was found to be 16%, 12% for
surgical consultants and 8% for surgical trainees [12]. Three different studies
evaluating residual rates from hospital in-patients also showed similar results
with rates of 13.73% [13], 14% [14] and 14% [12] respectively.
METHODOLOGY
The Human Resources and Ethics Committee (HREC) granted approval to the
Cancer Council of Victoria (CCV) on the 1/10/2008 by the Department of Health
and Ageing and was given the reference number 2008/CO004599. Ethics approval
was for the use of Medicare Australia (MA) data to be examined by the CCV for
epidemiological purposes. MA publishes
the total number of claims and benefits paid. These are made freely available
to the public. MA data relevant to treatment of recurrent and residual non
melanoma skin cancers were collected. The item numbers included: 31256, 31261, 31266,
31271, 31276, 31281, 31286, 31291, 31257, 31262, 31267, 31272, 31277, 31282,
31287, 31292, 31258, 31263, 31268, 31273, 31278, 31283, 31288, 31293, 31295.
Data were subdivided into three different groups: primary treatment,
residual treatment and recurrent treatments.
Each sub-group was then examined after stratification for state, age and
gender. Treatment services were also examined by provider type – i.e. the
number of specialists vs. the number of general practitioners (GPs) that
provided the treatment service.
Proportions of recurrent and residual non-melanoma skin cancers were
calculated.
RESULTS
For this study 2,607,119 services were extracted for use. Overall, MA
was billed most commonly for serial curettage, carbon dioxide laser or erbium
laser excision-ablation. For the
treatment of NMSC, 60% of item numbers were billed by male patients in the 70
-79 year-old age group.
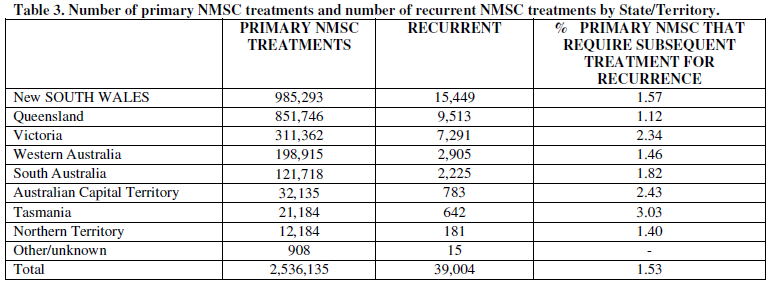
New South Wales had the highest number of NMSC treatments. Both New
South Wales and Queensland accounted for over 72.2% of medicare billings for
all NMSC treatments(including primary, recurrent and residual lesions). In
contrast the Australian Capital Territory, Northern Territory and Tasmania
required roughly 2.65% of Australia’s NMSC services.
Recurrent NMSC
A total of 39,004 recurrent NMSC treatments were billed between the
period of 2004-2007. Specialists accounted for
Overall, the percentage of primary NMSC treatments that required
subsequent treatment for a recurrence varied between states. Interestingly,
only 1.12 % of all primary
Age group trends seen in the recurrent treatment of NMSC demonstrated
that patients in the 70-79 year age group were the most likely patients to have
a recurrent NMSC. Patients aged between 60 -79 years old accounted for more
than half of the recurrent NMSC treatments. In the 50–79 year age group male
patients were more likely to have a recurrence, with males in the 60-69 year
age group almost twice as likely to have a recurrence compared to females.
Males accounted for 60% of services for treatment of recurrences.
Residual NMSC
Similar to recurrent NMSC, Queensland and New South Wales accounted for the bulk of residual NMSC treatments billed (63.7% combined) in Australia. South Australia and Western Australia billed similar numbers of NMSC residual treatments (2,643 and 2,128 respectively), despite Western Australia billing 56% more primary NMSCs than South Australia.
Overall, the proportion of NMSC requiring residual treatment was 1.26% (Table 4). Rates were lowest in New South Wales at 1.06% and highest in Australian Capital Territory at 2.42%.Sizing of recurrent
NMSC
Approximately 11,594 of original NMSC lesions requiring a second treatment for residual occurrence were under 10mm, representing over one half of the residual NMSC billed (Figure 1).
DISCUSSION
NMSC remains the most common cancer in Australia, yet there is limited
literature examining the trends in recurrent or residual NMSC.
This study is the first that reviews both recurrent and residual NMSC
within the whole of Australia using multiple treatment modalities.
The method of using MA data to evaluate the frequencies of residual and
recurrent NMSC has not been used to evaluate recurrence or incomplete
excisions. There have been no recent studies that have examined these figures
in Australia. Studies by Malhotra et al. [15] and Leibovitch et al. [16] examine
an Australia-wide databases, however the NMSC in these studies were excised
only by Mohs surgery.
MA item numbers chosen for this study were all relevant to NMSC. Each
billing code has a service ‘definition’ or criteria. For example item 31277
contains the following criteria: “Basal or
squamous cell carcinoma, residual, removal of, from face, neck (anterior to the sternomastoid muscles) or lower leg (mid
calf to ankle), where performed
by a practitioner other than the practitioner who provided the previous
treatment, where the
original tumour size was more than 20mm in diameter and where
removal is by surgical excision
(other than by shave excision) and suture and where the specimen
excised is sent for histological examination”. Unfortunately since each
of the item number ‘definitiions’ assigned by Medicare include either Basal
cell or squamous cell carcinoma in the definition, it was not possible to
determine what type of NMSC was treated at the visit .
The proportion of recurrences (8%) predicted in a study by Czarnecki et
al. (1996) were more than four times higher than the rates predicted in this
chapter (1.54%), which was an unexpected result. All patients seen in the study
by Czarnecki et al. [17] were seen by one doctor in a private practice and a
public hospital every 3-6 months. Factors such as specialist treatment and
participant selection are potential biases. Presumably, specialist treatment
would result in increased accuracy of detecting both new and recurrent NMSCs. Given
the quarter-yearly follow-up, it is likely that a larger number of recurrences
were picked up by Czarnecki [17] compared to routine examination by a patient’s
regular practitioner and recorded by MA. This discrepancy may suggest that
providers are not accurately picking up recurrences of NMSC in the wider
population, or that providers are under-reporting NMSC recurrence treatments to
MA, reporting these as primary treatments instead.
Residual NMSC rates in Australia, ranged within the
literature, between 0.7% and 24.5%, while rates for recurrence ranged between
0.7 and 17% [5,15-27]. There are a
number of reasons for these discrepencies. Overall, the studies did not use a
sample population that was representative of all NMSC lesions. For example, in some studies, lesions
examined were obtained from specialist referral centres, specialist clinics or
GP-run clinics. Lesions excised by specialists were more likely to have a lower
residual and recurrence rate compared to lesions excised by GPs. One study
examined reports from a single pathologist who received excised lesions from
rural and metropolitan Western Australia. This was the only study that examined
lesionsfrom all specialist types and GPs [28].
Studies by Malhotra et al. and Leibovitch et al. examined
recurrence and residual rates in the entire Australian population. Data for
these studies were extracted from the database for Skin and Cancer Foundation
of Australia [5,15,18,22,26]. However, the estimated rates were for lesions
treated with Mohs surgery. Some of the studies examined rates within one body
location or lesions with perineural invasion [16,18].
The rates for both recurrence and residual NMSC vary in
both the Australian studies and in the studies performed overseas. Furthermore, most studies in Australia
examined reports from surgically excised lesions, with only one study which
examined a variety of treatments within a specialist referral centre [29].
Whilst the studies led by Leibovitch et al. [5,16,18,19,22] and Malhotra et al.
[25-27] examined lesions from the entire Australian population, they focused on
only one treatment modality. There are no other studies that examine recurrent
and residual NMSC in the entire population. Access to the MA data set allows
for a novel approach in exploring residual and recurrent NMSCs in the Australian
population that have been treated with a variety of modailities.
This study also revealed that lesions under 10mm in diameter were more
likely to require a second excision for residual NMSC. One suggested reason is
that larger lesions may be treated with larger margins to ensure that the whole
lesion is excised, where as smaller margins are more likely to be used for
smaller lesions. The results of this study may potentially dictate future
guidelines on the treatment options for NMSC and may prompt further review of
the recommended excision margins for smaller lesions.
A limitation of this study was that there was no record of the initial
lesion the recurrence was associated with.
For example, in a patient with several primary lesions excised over the
last month, there was no way of identifying which primary lesions developed the
recurrence. The time frame for recurrences was therefore unable to be
calculated.
Another limitation of examining the recurrent and residual NMSC
databases are that the assumption was made that providers billed MA correctly.
While there is no financial incentive to bill a recurrent lesion as a primary
NMSC, it is a possibility that physicians may not remember the characteristics
of the original primary due much time passing between the primary and
recurrence. This would explain the low
numbers of residual and recurrent billing data for NMSC. Given that the
Medicare definitions contained arbitrary groupings of NMSC body locations (e.g.
item 31256 is used for NMSC on the nose, eyelid, lip, ear, digit or genital),
it was not possible to analyse body location trends and produce results that
could be interpreted.
Furthermore, recurrences may take years to develop and there is a
possibility that a clinician would bill the recurrence as another primary
lesion rather than a recurrent lesion. This study was based on the assumption
that residual and recurrent lesions were accurately billed to MA.
Unfortunately, body locations of each NMSC lesion were not recorded by MA and therefore
rates of residual and recurrent lesions could not be calculated for each body
part.
This study focused on rates of residual and recurrent NMSC rates within
Australia and in each state. The Medicare data has the potential to examine
these trends further at a Local Government Area (LGA) level. Further studies
could then examine if differences in rates lie within rural and urban
populations, and whether this difference is a reflection of the experience of
the healthcare providers. Furthermore, with the rise of GP-led skin clinics in
Australia, future monitoring of rates within these clinics could be examined in
more depth.
Due to the limitations in the Medicare dataset, body locations were not
able to be obtained. Hence, distinguishing between cryotherapy, electrocautery
and dessication and laser was not possible. Studies that examine rates of
recurrence in lesions that have initially been treated using these modalities
have not been conducted in Australia. Future research could be conducted on a smaller
scale to establish rates in Australia for each treatment modality and to make
recommendations in the future regarding their use in the treatment of NMSC.
In brief, this study examines the proportion of
residual and recurrent cases being billed to MA. This is the first study which
examines rates throughout Australia. While most studies examine recurrence
rates after surgical excision, this study takes into account recurrences using
ablative techniques.
REFERENCES
1. Perera E, Gnaneswaran N, Staines C, Win AK, Sinclair R (2015) Incidence and prevalence of non-melanoma skin cancer in Australia: A systematic review. Australas J Dermatol
2. Fransen M, Karahalios A, Sharma N, English DR, Giles GG, et al. (2012) Non-melanoma skin cancer in Australia. Med J Aust 197: 565-568.
3. Emmett AJ, Broadbent GG (1981) Basal cell carcinoma in Queensland. Aust N Z J Surg 51: 576-590.
4. Palmer VM, Wilson PR (2013) Incompletely excised basal cell carcinoma: residual tumor rates at Mohs re-excision. Dermatol Surg 39: 706-718
5. Leibovitch I, Huilgol SC, Selva D, Richards S, Paver R (2005) Basal cell carcinoma treated with Mohs surgery in Australia II. Outcome at 5-year follow-up. J Am Acad Dermatol 53: 452-457.
6. Chren MM, Torres JS, Stuart SE, Bertenthal D, Labrador RJ, et al. (2011) Recurrence after treatment of nonmelanoma skin cancer: a prospective cohort study. Arch Dermatol 147: 540-546
7. Schmook T, Stockfleth E (2003) Current treatment patterns in non-melanoma skin cancer across Europe. J Dermatol Treat 3: 3-10.
8. Braathen LR, Szeimies RM, Basset-Seguin N, Bissonnette R, Foley P, Pariser D, et al. (2007) Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: an international consensus. International Society for Photodynamic Therapy in Dermatology, 2005. J Am Acad Dermatol 56: 125-43.
9. Rieger KE, Linos E, Egbert BM, Swetter SM (2010) Recurrence rates associated with incompletely excised low-risk nonmelanoma skin cancer. J Cutan Pathol 37: 59-67.
10. Sussman LA, Liggins DF (1996) Incompletely excised basal cell carcinoma: a management dilemma? Aust N Z J Surg 66: 276-278.
11. Corwin P, Munn E, Nicholls D (1997) A study of general practitioners' skin surgery in Canterbury. N Z Med J 110: 253-255.
12. Talbot S, Hitchcock B (2004) Incomplete primary excision of cutaneous basal and squamous cell carcinomas in the Bay of Plenty. N Z Med J 117: U848.
13. Schreuder F, Powell BW (1999) Incomplete excision of basal cell carcinomas: an audit. Clin Perform Qual Health Care 7: 119-120.
14. Bhatti AZ, Asif S, Alwan M (2006) Factors affecting incomplete excision of nonmelanoma skin cancers in New Zealand. Ann Plast Surg 57: 513-516.
15. Malhotra R, Huilgol SC, Huynh NT, Selva D (2004) The Australian Mohs database, part I: periocular basal cell carcinoma experience over 7 years. Ophthalmology 111: 624-630.
16. Leibovitch I, Huilgol SC, Selva D, Richards S, Paver R (2005) Basal cell carcinoma treated with Mohs surgery in Australia III. Perineural invasion. J Am Acad Dermatol 53: 458-463.
17. Czarnecki D, Staples M, Mar A, Giles G, Meehan C (1996) Recurrent nonmelanoma skin cancer in southern Australia. Int J Dermatol 35: 410-412.
18. Leibovitch I, Huilgol SC, Selva D, Hill D, Richards S, et al. (2005) Cutaneous squamous cell carcinoma treated with Mohs micrographic surgery in Australia II. Perineural invasion. Journal of the American Academy of Dermatol 53: 261-266.
19. Leibovitch I, Huilgol SC, Selva D, Hill D, Richards S, et al. (2005) Cutaneous squamous cell carcinoma treated with Mohs micrographic surgery in Australia I. Experience over 10 years. Journal of the American Academy of Dermatology 53: 253-260.
20. Leibovitch I, Huilgol SC, Selva D, Lun K, Richards S, et al. (2005) Microcystic adnexal carcinoma: treatment with Mohs micrographic surgery. J Am Acad Dermatol 52: 295-300.
21. Leibovitch I, Huilgol SC, Selva D, Paver R, Richards S (2005) Cutaneous lip tumours treated with Mohs micrographic surgery: clinical features and surgical outcome. Br J Dermatol 153: 1147-1152.
22. Leibovitch I, Huilgol SC, Selva D, Richards S, Paver R (2005) Basal cell carcinoma treated with Mohs surgery in Australia I. Experience over 10 years. J Am Acad Dermatol 53: 445-451.
23. Leibovitch I, Huilgol SC, Selva D, Richards S, Paver R (2005) Basosquamous carcinoma: treatment with Mohs micrographic surgery. Cancer 104: 170-175.
24. Leibovitch I, Huilgol SC, Selva D, Richards S, Paver R (2005) Cutaneous squamous carcinoma in situ (Bowen's disease): treatment with Mohs micrographic surgery. J Am Acad Dermatol 52: 997-1002.
25. Malhotra R, Huilgol SC, Huynh NT, Selva D (2004) The Australian Mohs database, part II: periocular basal cell carcinoma outcome at 5-year follow-up. Ophthalmology 111: 631-636.
26. Malhotra R, Huilgol SC, Huynh NT, Selva D (2004) The Australian Mohs database: periocular squamous cell carcinoma. Ophthalmology 111: 617-623.
27. Malhotra R, James CL, Selva D, Huynh N, Huilgol SC (2004) The Australian Mohs database: periocular squamous intraepidermal carcinoma. Ophthalmology 111: 1925-1929.
28. Rippey JJ, Rippey E (1997) Characteristics of incompletely excised basal cell carcinomas of the skin. Med J Aust 166: 581-583
29. Ashby MA, Smith J, Ainslie J, McEwan L (!989) Treatment of nonmelanoma skin cancer at a large Australian center. Cancer 63: 1863-1871.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4



QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Alcoholism Clinical Research
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- Journal of Spine Diseases
- Journal of Cell Signaling & Damage-Associated Molecular Patterns
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Clinical Trials and Research (ISSN:2637-7373)


