1668
Views & Citations668
Likes & Shares
Pagetoid spread of anal canal carcinoma is a rare
phenomenon, mimicking perianal primary extra-mammary Paget's disease. We report
two cases with perianal pagetoid spread associated with submucosally invasive
adenocarcinoma in the anal canal. Both cases presented at our hospital with perianal
skin lesions. In each case, histological examination of the biopsied specimens
from the lesions revealed that Paget cells had infiltrated all levels of the
epidermis. The tumor cells were positive for CK7 and CK20, but negative for
GCDFP-15. According to a diagnosis in both cases of anal canal carcinoma by endoscopic
examination, one patient underwent laparoscopic abdominoperineal resection and
extensive lymph node dissection, and the other patient received preoperative
radiotherapy, rectal amputation and lymphadenectomy. In both cases, a diagnosis
of primary anal canal carcinoma was made by skin biopsy of the lesions as
pagetoid spread. Immunohistochemical analysis was helpful in the differential
diagnosis between primary Paget’s disease and pagetoid spread with anorectal
carcinoma. Furthermore, we found that management of perianal Paget’s disease is
necessary for estimating prognosis and selecting appropriate treatment
according to the patient’s condition.
INTRODUCTION
Pagetoid spread of anal canal carcinoma is a rare phenomenon, mimicking perianal primary extra-mammary Paget's disease (EMPD). EMPD is thought to be an epidermotropic neoplasm arising from the apocrine glands of extra-mammary organs such as the valve, penis scrotum, perineum, axilla, and perianal region [1-3]. On the other hand, pagetoid spread occurs in cases of anal canal, rectal, cervical, and bladder carcinomas [4-7]. Specifically, perianal pagetoid spread is suggested to be skin infiltration of anal canal carcinoma or rectal carcinoma [4-5]. We report two cases with perianal pagetoid spread associated with submucosally invasive adenocarcinoma in the anal canal.
REPORT
OF CASES
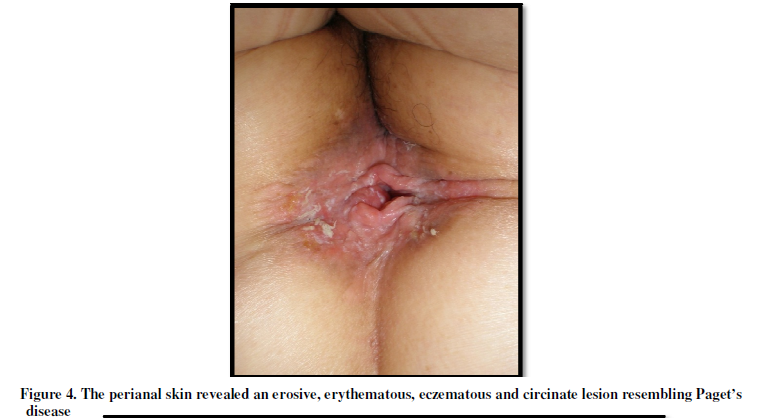
Case 1: A 64-year-old woman was referred
to our hospital with a one-year history of a well-marginated, erosive, erythematous
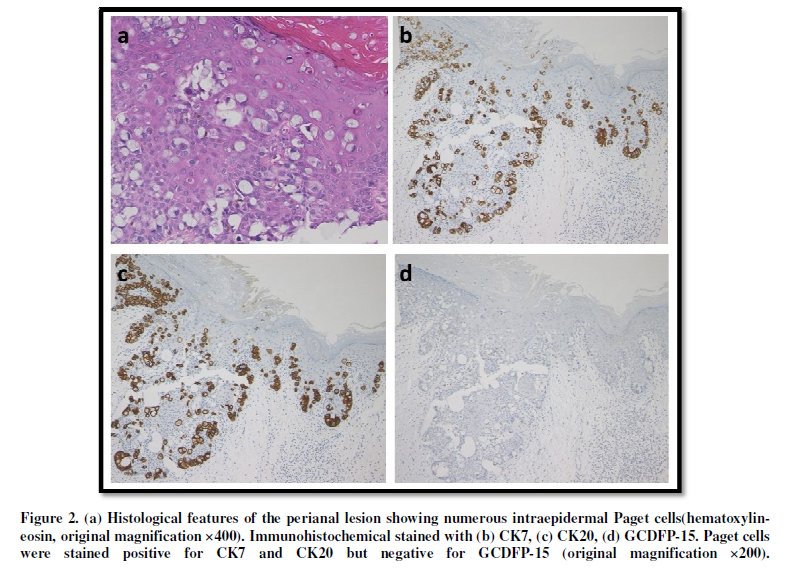
plaque with pain and itchiness on the perianal skin (Figure 1). Histological
examination of the biopsiedspecimens from the lesion revealed large atypical
cells with ample pale-staining cytoplasm, pleomorphic nuclei, and occasional
prominent nucleoli, indicative of Paget cells. Tumor cells infiltrated throughout
all levels of the epidermis (Figure 2a). Immunohistochemical staining of the
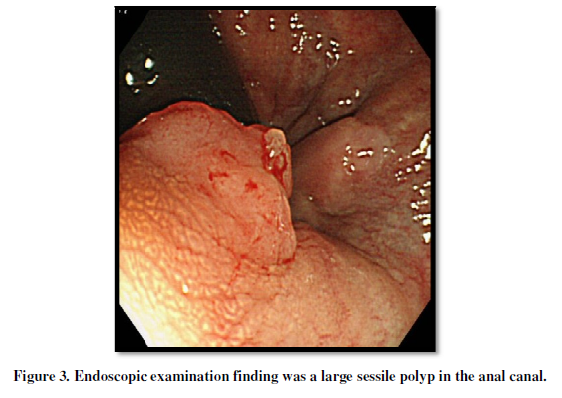
cells was positive for CK7 and CK20, but negative for GCDFP-15 (Figure 2b-d). Endoscopic
examination showed a large sessile polyp in the anal canal, and normal findings
above the dentate line (Figure 3). The patient underwent
laparoscopicabdominoperineal resection and extensive lymph node dissection, and
was diagnosed as having anal canal carcinoma.
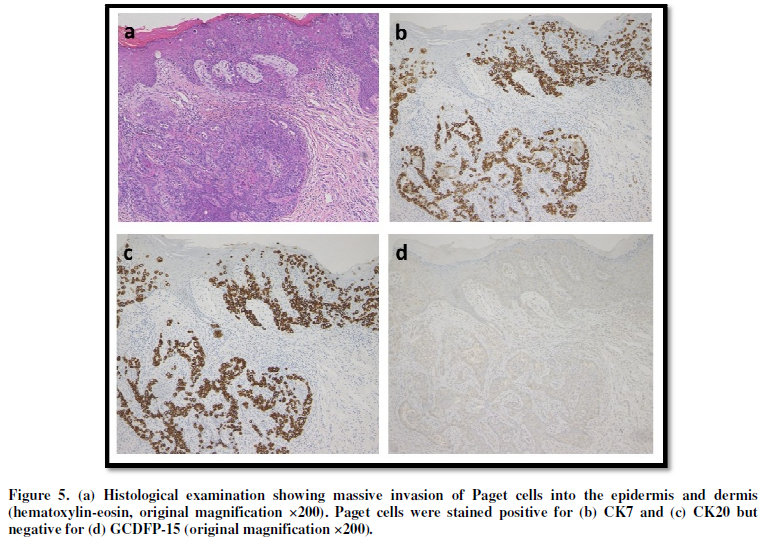
Skin biopsy showed the invasion of Paget cells, which formed nests in
the epidermis and dermis. The tumor cells were strongly positive for CK7 and
CK20, but negative for GCDFP-15 (Figure 5). Proctoscopic examination showed a
large polypoid lesion on the anal canal, but no abnormal findings in the
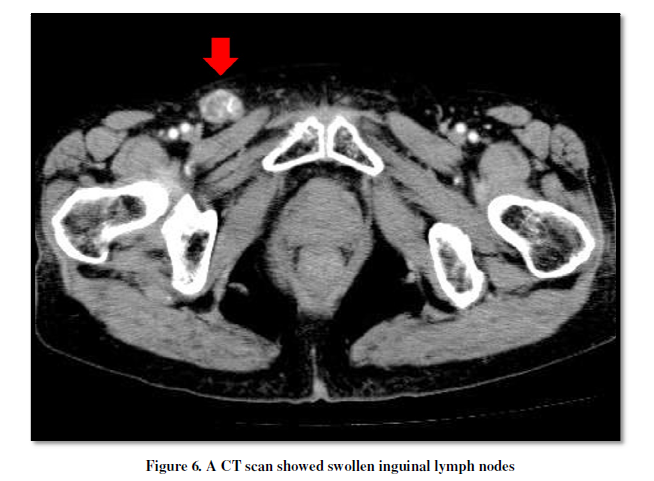
anterior wall from the dentate line. A CT scan revealed swollen inguinal lymph
nodes (Figure 6). The patient was treated with preoperative radiotherapy for
both Paget’s disease and anal canal carcinoma, as well as rectal amputation and
lymphadenectomy of the swollen lymph nodes.
DISCUSSION
Perianal Paget’s disease is rare and often associated with anorectal
malignancy. The cases of anorectal carcinoma with Pagetoid spread have been
reported as extra-mammary secondary perianal Paget’s disease. Helwig EB et
alreported that sevenof 40 patients with perianal Paget’s disease had primary
internal or extracutaneous malignancy and four of those seven patients had
concomitant rectal adenocarcinoma [8]. In another report, 33% of the perianal
Paget’s disease cases coexisted with anorectal carcinoma [4].
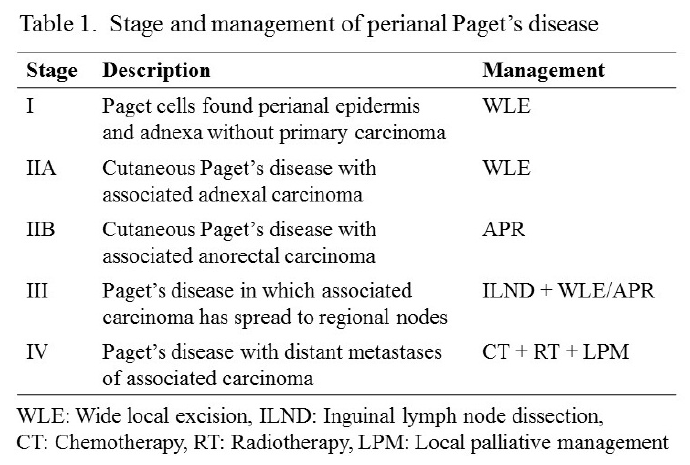
The treatment of perianal Paget’s disease is recommended by many
oncologists to be selected in accordance to each stage (Table 1) [2]. According
to this staging system, our Case 1 was grouped as stage IIB and abdominoperineal
resection should be recommended. This patient was additionally treated with
regional lymph node dissection. Case 2 was grouped as stage III and inguinal
lymph node dissection with wide local excision or abdominoperineal resection. The
treatment which with preoperative radiotherapy, rectal amputation and
lymphadenectomy of swollen lymph nodes as a palliative treatment was selected
with consideration for the patient’s quality of life. Recently, some reports
revealed that molecular targeted drugs, such as bevacizumab (VEGF inhibitor)
and ceuximab (EGFR inhibitor), were effective against advanced rectal carcinoma
[13-14] and may also improve the prognosis of the patients with Pagetoid spread
lesion.
REFERENCES
1. Jones RE, Austin C, Ackerman AB (1979) Extramammary Paget's disease. A critical reexamination. Am J Dermatopathol 1:101-32.
2. Hart WR, Millman JB (1977) Progression of intraepithelial Paget's disease of the vulva to invasive carcinoma. Cancer 40: 2333-2337.
3. Wick MR, Goellner JR, Wolfe JT 3rd, Su WP (1985) Vulvar sweat gland carcinomas. Arch Pathol Lab Med 109: 43-47.
4. Goldman S, Ihre T, Lagerstedt U, Svensson C (1992) Perianal Paget's disease: report of five cases. Int J Colorectal Dis 7: 167-169.
5. Suenaga M, Oya M, Ueno M, Yamamoto J, Yamaguchi T, Mizunuma N, Hatake K, Kato Y, Muto T (2006) Anal canal carcinoma with Pagetoid spread: report of a case. Surg Today 36: 666-669.
6. Mahdi H, Thrall M, Agoff N, Doherty M (2011) Pagetoid adenocarcinoma in situ of the cervix with pagetoid spread into the vagina. Obstet Gynecol 118: 461-463.
7. Salamanca J, Benito A, García-Peñalver C, Azorín D, Ballestín C, et al. (2004) Paget's disease of the glans penis secondary to transitional cell carcinoma of the bladder: a report of two cases and review of the literature. J Cutan Pathol 31: 341-345.
8. Helwing EB, Graham JH (1963) Anogenital (extramammary) Paget's disease. A clinicopathological study. Cancer 16: 387-403.
9. Ohnishi T, Watanabe S (2000) The use of cytokeratins 7 and 20 in the diagnosis of primary and secondary extramammary Paget's disease. Br J Dermatol 142: 243-247.
10. Haga R, Suzuki H (2003) Rectal carcinoma associated with pagetoid phenomenon. Eur J Dermatol 13: 93-94.
11. Ramalingam P, Hart WR, Goldblum JR (2001) Cytokeratin subset immunostaining in rectal adenocarcinoma and normal anal glands. Arch Pathol Lab Med 125: 1074-1077.
12. Shutze WP, Gleysteen JJ (1990) Perianal Paget's disease. Classification and review of management: report of two cases. Dis Colon Rectum 33: 502-507.
13. Fornaro L, Caparello C, Vivaldi C, Rotella V, Musettini G, et al. (2014) Bevacizumab in the pre-operative treatment of locally advanced rectal cancer: a systematic review. World J Gastroenterol 20: 6081-6091.
14. Folprecht G, Gruenberger T, Bechstein WO, Raab HR, Lordick F, et al. (2010) Tumour response and secondary resectability of colorectal liver metastases following neoadjuvant chemotherapy with cetuximab: the CELIM randomised phase 2 trial. Lancet Oncol 11: 38-47.
15. Lian P, Gu WL, Zhang Z, Cai GX, Wang MH, et al. (2010) Retrospective analysis of perianal Paget's disease with underlying anorectal carcinoma. World J Gastroenterol 16: 2943-2948.
16. Marchesa P, Fazio VW, Oliart S, Goldblum JR, Lavery IC, et al. (1997) Long-term outcome of patients with perianal Paget's disease. Ann Surg Oncol 4: 475-480.
-
 Table 1
Table 1

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Oncology Clinics and Research (ISSN: 2643-055X)
- Journal of Spine Diseases
- Journal of Clinical Trials and Research (ISSN:2637-7373)
- Journal of Cardiology and Diagnostics Research (ISSN:2639-4634)
- Journal of Forensic Research and Criminal Investigation (ISSN: 2640-0846)
- Ophthalmology Clinics and Research (ISSN:2638-115X)


