1068
Views & Citations68
Likes & Shares
Background: There is an association between psoriasis and metabolic syndrome
(MetS). Desnutrin is a lipase found in the adipose tissue of mice that
increases lipolysis, fatty acid oxidation within adipose tissue, and
thermogenesis, resulting in higher energy expenditure and resistance to
obesity.
Objective: We examined the
desnutrin levels in patients with psoriasis and their association with insulin
resistance and MetS.
Methods: This study enrolled
30 patients with psoriasis and 30 controls. Fasting blood glucose, serum
lipids, insulin, C-reactive peptide, and desnutrin levels were measured. The extent
and severity of lesions were determined using the Psoriasis Area and Severity
Index (PASI) and body surface area (BSA) involvement.
Results: The mean serum
desnutrin level in the patients with psoriasis (9.02 ± 1.90) was significantly
(p = 0.04) lower than in the controls (10.66 ± 3.86). The mean serum desnutrin
levels in individuals with MetS were similar to individuals without MetS.
Conclusion: Serum desnutrin levels in patients with psoriasis were lower than those
of the controls. In addition, low serum desnutrin levels were not associated
with MetS or insulin resistance in our study. This may be due to the low number
of patients with MetS or insulin resistance or due to the actual low serum
desnutrin levels.
Keywords: Psoriasis,
Desnutrin, Insulin resistance, Metabolic syndrome
INTRODUCTION
The prevalence rates of metabolic syndrome
(MetS), subclinical atherosclerosis, cardiovascular risk factors, diabetes,
hypertension, dyslipidaemia, and obesity are higher among patients with
psoriasis than they are in the general population [1,2]. The association between psoriasis and MetS
is thought to be related to chronic inflammation [3]. Increased proinflammatory
cytokines in chronic inflammation result in atherogenesis and peripheral
insulin resistance, which in turn cause hypertension and a tendency towards
type 2 diabetes [4,5]. Life expectancy is shortened in patients with
psoriasis, largely due to cardiovascular disease [6].
Desnutrin, also called adipose triglyceride
lipase, is a recently discovered peptide hormone. It is found primarily in
adipose tissue and in lesser amounts in other tissues. Fasting and
glucocorticoids stimulate the release of desnutrin [7,8].
Desnutrin is the major triglyceride lipase in
the adipose tissue of rats and decreases the storage of triacylglycerol, while
it increases fatty acid oxidation and thermogenesis by increasing lipolysis
when released in excess. Therefore, it results in resistance to diet-related
obesity [8-10]. Whenever lipolysis in adipose tissue is altered,
triacylglycerol is stored and free fatty acids are increased. This provides a
basis for serious metabolic conditions such as insulin resistance, type 2
diabetes, hypertension, cardiovascular diseases, and obesity [11-13].
This study investigated the serum desnutrin
levels in patients with psoriasis and their association with insulin resistance
and MetS.
MATERIALS AND METHODS
Study Design
This study enrolled 30 patients with psoriasis
and 30 healthy controls. The study was approved by the local ethics committee
and and informed consent was obtained from all participants. Exclusion criteria
were as follows: age <18 years, systemic disease (diabetes, hypothyroidism,
or hyperthyroidism), pregnancy, malignancy, and systemic drug or alcohol abuse.
Age, gender, height, weight, and waist circumferences were recorded. Body mass
index [BMI= weight (kg)/height2 (m2)] was calculated and
obesity was determined according to the World Health Organisation
classification as follows: normal range (18.5–24.9 kg/m2), grade 1
overweight (25.0–29.9 kg/m2), grade 2 overweight (30.0–39.9 kg/m2),
and grade 3 overweight (≥ 40.0 kg/m2). A BMI > 30 was deemed to
represent obesity [14].
The severity of psoriasis was assessed using
the Psoriasis Area and Severity Index (PASI) and percent body surface area
(BSA) involvement [15]. Quality of life was evaluated using the Dermatology
Life Quality Index (DLQI), which Ozturkcan et al. validated in Turkish [16].
Laboratory Assessment
Fasting blood glucose, total cholesterol,
low-density lipoprotein (LDL), very-low-density lipoprotein (VLDL),
high-density lipoprotein (HDL), triglyceride, insulin, and C-peptide levels
were measured. The homeostasis model assessment of insulin resistance (HOMA-IR
= [insulin (mU/L) × glucose (mmol/L)] / 22.5) was used to calculate insulin
resistance [17]. MetS was diagnosed using the International Diabetes Foundation
criteria as obesity in the presence of two or more of the following clinical
features: fasting blood glucose ≥ 100 mg/dL; hypertriglyceridemia ≥ 150 mg/dL,
HDL < 40 mg/dL in males or < 50 mg/dL in females; blood pressure ≥ 130/85
mm Hg; and waist circumference ≥ 94 cm in males or ≥ 80 cm in females [18].
Collection and storage of blood samples
As desnutrin is a peptide hormone, in order to
prevent proteolysis, aprotinin (500 kallikrein units/mL) was added to untreated
collection tubes before collecting blood samples. Samples were collected at
9-10 a.m. after an overnight fast to avoid any confounding effects associated
with circadian rhythms. Samples (5 mL) were collected and centrifuged at 3000 ×
g for 5 min. The serum was transferred to microcentrifuge tubes and frozen at
–80°C until analysis. Serum desnutrin levels were determined using an
enzyme-linked immunosorbent assay (ELISA), according to the manufacturer’s
protocol (CUSABİO; cat. no: CSBE12688h, lot: N17060631) using a commercial
ELISA kit (Wuhan; P.R. China). The inter- and intra-assay coefficients of
variation were < 8.1% and <7.0%, respectively. The minimum detectable
dose of human desnutrin is 1.56 mIU/ml, while maximum detectable dose of human
desnutrin is 400 mIU/ml.
STATISTICAL ANALYSIS
The statistical analysis was performed using
SPSS ver. 22.0. The data obtained in the study were expressed as means ± SD.
The independent samples t-test and Mann–Whitney U-test were used to compare the
groups. Differences with p < 0.05 were accepted as statistically
significant.
RESULTS
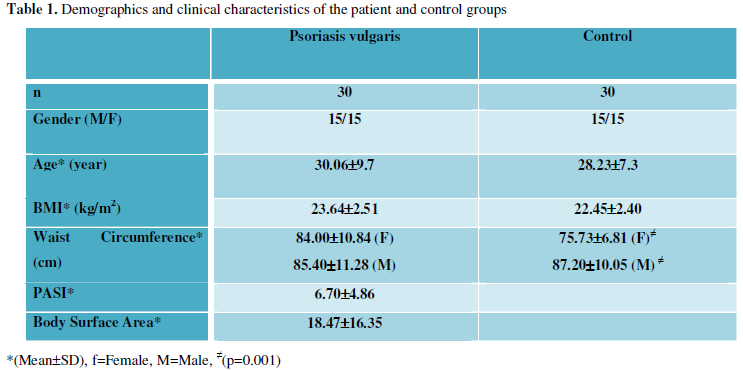
The mean age of the psoriasis patients and
controls was 30.06 ± 9.7
(range 18–55) and 28.23 ± 7.3
(range 18–45) years, respectively. There were no significant differences in
mean age, BMI, or gender distribution between the groups. Table 1 summarises the demographic and clinical characteristics of
the patient and control groups.
In the psoriasis group, the mean duration of
the disease was 10.23 ± 6.00
(range 1–22) years. There was nail involvement in 15 (50.0%) patients, genital
mucosa involvement in six (20.0%), and scalp involvement in 24 (80.0%).
The mean serum desnutrin level was
significantly (p = 0.04) lower in the patient group (9.02 ± 1.90 mIU/mL) than
in the controls (10.66 ± 3.86 mIU/mL). Table
2 summarises the laboratory findings of the patient and the control groups.
Increased insulin resistance was found in seven
(23.3%) patients and three (10.0%) controls. There was no significant
difference between the mean serum desnutrin level of the patients with insulin
resistance (8.73 ± 0.60 mIU/mL) and those without insulin resistance (9.11 ±
2.15 mIU/mL).
Twelve patients (40.0%) and 10 controls (33.3%)
were diagnosed with MetS. The mean serum desnutrin level in the patients with
MetS and without MetS was 9.37 ± 2.84 and 8.79 ± 0.90 mIU/mL, respectively. The
mean serum desnutrin level in the controls with and without MetS was 10.00 ±
2.48 and 10.99 ± 4.41 mIU/mL, respectively. The mean desnutrin levels in
individuals with MetS (9.65 ± 2.64 mIU/mL) and without MetS (9.95 ± 3.41
mIU/mL) in both the patient and control groups were similar. Patients with
psoriasis with or without MetS were compared with respect to BSA involvement,
PASI, and DLQI. The duration of the disease (13.91 ± 4.48 years) and BSA
involvement (24.47 ± 16.57%) of the patients with MetS were significantly
higher than those of the patients without MetS (7.77 ± 5.71 years and 14.48 ±
15.36%, respectively) (p = 0.005 and p = 0.04, respectively).
The mean serum
desnutrin level was higher in men (10.40 ± 4.03 mIU/mL) than in women (8.54 ±
0.39 mIU/mL); however, the difference was not significant. There was also no
significant association between the BMI, BSA, PASI score and mean desnutrin
level.
DISCUSSION
Desnutrin increases
lipolysis by decreasing the secretion of insulin during a prolonged fast [19].
Insulin is also a powerful antilipolytic hormone and inhibits lipolysis in the
postprandial state [20]. Desnutrin increases the sensitivity to insulin by
increasing fatty acid oxidation and energy use in adipocytes [9]. The
inhibition of the activity of desnutrin by insulin contributes to the
development of obesity, insulin resistance, and hyperlipidaemia [13]. In one
study, patients with MetS were fed diets containing different proportions of
fat for 12 weeks. At the end of the diet intervention, desnutrin gene synthesis
was increased in both the fasting and postprandial periods in the adipose
tissue of individuals who were on a high-fat diet. Increased desnutrin
synthesis csombined with increased glucose, insulin resistance, and HOMA-IR
levels in patients with MetS has been explained by corruption of the
suppressive function of insulin on desnutrin by saturated fatty acids [21].
Another study reported that the lipolytic activity of desnutrin in adipocytes
after fatty meals decreased at the end of the postprandial period due to the
inhibitory effect of insulin on intracellular lipase [22]. These studies
involved diet interventions. However, it was also reported that desnutrin gene
synthesis in the adipose tissue in patients with MetS continued without being
affected by changes in the fat composition of the diet, and the gene synthesis
was reported to increase after consuming low-fat, high-carbohydrate diets [23].
In obese individuals,
desnutrin increases due to inflammation in adipose tissue and decreases after
weight loss [24]. Similarly, in a study of 28 patients, the patients lost
weight while on a low-energy diet for 2 months and they were followed for 10
months with the goal of preserving their post-diet weights. The desnutrin level
in adipose tissue during the weight-loss period was positively correlated with
weight loss; however, the desnutrin level increased during the 10-month
follow-up period [25]. Camargo et al. found a positive correlation between
desnutrin mRNA levels in the fasting state after a dietary intervention period
and BMI [21].
A few studies have
analysed serum desnutrin levels. Demir et al. found a positive correlation
between the levels of serum fasting insulin and desnutrin in patients with acne
vulgaris [26]. In a study comparing 66 patients with diabetes and 48 obese,
overweight, or normal weight individuals with normal glucose tolerance, Yang et
al. reported that serum fasting desnutrin levels were lower in obese or
overweight individuals compared to the normal weight individuals, including
those with type 2 diabetes, and that desnutrin levels were negatively
correlated with HOMA-IR, triglycerides, and BMI [27]. In our study, no
significant associations were found among psoriasis patients between decreased
serum desnutrin levels and MetS, insulin resistance, HOMA-IR, or BMI. Serum
desnutrin levels may have been affected by inflammatory processes, in addition
to metabolic factors.
In psoriasis,
proinflammatory cytokines, such as IL-6 and TNF-α, increase locally and
systemically [28]. Inflammation and, in particular, TNF-α have been reported to
increase lipolysis [29]. Camargo et al. observed that desnutrin gene synthesis
affected lipid metabolism and inflammatory markers and they also reported a
positive correlation between desnutrin mRNA levels in adipose tissue and
fasting and postprandial plasma TNF-α concentrations after completion of the
diet intervention [21].
Desnutrin is a newly
discovered molecule and its functions are affected by many factors, such as
inflammatory processes, fasting-satiety, a fatty diet, and insulin. Analyses of
the desnutrin levels in adipose tissue have demonstrated that desnutrin is an
adipokine and its rate of synthesis in adipose tissue is not fully reflected in
the serum. In this study, we also encountered difficulty measuring the serum
desnutrin with an ELISA method, since its serum levels are very low.
In conclusion, the
level of desnutrin, which has an important role in carbohydrate and fat
metabolism, was significantly lower in psoriasis patients in this study. It was
not directly related to MetS or insulin resistance, possibly due to the low
number of patients with MetS or insulin resistance or due to the low serum
desnutrin levels observed in the study. Desnutrin level helped to distinguish
patients with psoriasis from control subjects. Therefore, we believe that
desnutrin may serve as a circulating bio-marker reflecting the inflammatory
condition in psoriasis. Larger controlled studies should evaluate the
relationship between desnutrin and psoriasis as well as other inflammatory
diseases.
ACKNOWLEDGEMENTS
Financial support: None
Conflict of interest: None
- Karoli R, Fatima J, Shukla V, et al. (2013) A study of
cardio-metabolic risk profile in patients with psoriasis. J Assoc
Physicians India 61: 798-803.
- Neimann AL, Shin DB, Wang X, et al. (2006) Prevalence of
cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol
55: 829-835.
- Padhi T (2013) Metabolic syndrome and skin: psoriasis and beyond.
Indian J Dermatol 58: 299-305.
- Henseler T, Christophers E (1995) Disease concomitance in psoriasis.
J Am Acad Dermatol 32: 982-986.
- Sommer DM, Jenisch S, Suchan M, et al. (2006) Increased prevalence
of the metabolic syndrome in patients with moderate to severe psoriasis.
Arch Dermatol Res 298: 321-328.
- Abuabara K, Azfar RS, Shin DB, et al. (2010) Cause-specific
mortality in patients with severe psoriasis: a population-based cohort
study in the U.K. Br J Dermatol 163: 586-592.
- Zimmermann R, Strauss JG, Haemmerle G, et al. (2004) Fat
mobilization in adipose tissue is promoted by adipose triglyceride lipase.
Science 306: 1383-1386.
- Villena JA, Roy S, Sarkadi-Nagy E, et al. (2004) Desnutrin, an
adipocyte gene encoding a novel patatin domain-containing protein, is
induced by fasting and glucocorticoids: ectopic expression of desnutrin
increases triglyceride hydrolysis. J Biol Chem 279: 47066-47075.
- Ahmadian M, Duncan RE, Varady KA, et al. (2009) Adipose
Overexpression of Desnutrin Promotes Fatty Acid Utilization and Attenuates
Diet-induced Obesity. Diabetes 58: 855-866.
- Lake AC, Sun Y, Li JL, et al. (2005) Expression, regulation, and
triglyceride hydrolase activity of Adiponutrin family members. J Lipid Res
46: 2477-2487.
- Ahmadian M, Duncan RE, Jaworski K, Sarkadi-Nagy E, Sul HS (2007)
Triacylglycerol metabolism in adipose tissue. Future Lipidol 2: 229-37.
- Unger RH (2002) Lipotoxic diseases. Annu Rev Med 53: 319-336.
- Kralisch S, Klein J, Lossner U, et al. (2005) Isoproterenol, TNF
alpha, and insulin downregulate adipose triglyceride lipase in 3T3-L1
adipocytes. Mol Cell Endocrinol 240: 43-49.
- WHO (1995) Physical status: the use and interpretation of anthropometry:
report of a WHO expert committee. WHO Tech Rep Ser 854: 1-452.
- Henseler T, Schmitt-Rau K (2008) A comparison between BSA, PASI,
PLASI, and SAPASI as measures of disease severity and improvement by
therapy in patients with psoriasis. Int J Dermatol 47: 1019-1023.
- Ozturkcan S, Ermertcan AT, Eser E, Sahin MT (2006) Cross validation
of the Turkish version of dermatology life quality index. Int J Dermatol
45: 1300-1307.
- Matthews DR, Hosker JP, Rudenski AS, et al. (1985) Homeostasis model
assessment: insulin resistance and beta-cell function from fasting plasma
glucose and insulin concentrations in man. Diabetologia 28: 412-419.
- Prodromas IS, Stylionos S, Dimitros T (2008) Metabolic syndrome in
rheumatic diseases: epidemiology, pathophysiology, and clinical
implications. Arthritis Research and Therapy 2008; 10: 207.
- Boden G, Shulman GI (2002) Free fatty acids in obesity and type 2
diabetes: defining their role in the development of insulin resistance and
betacell dysfunction. Eur J Clin Invest 32: 14-23.
- Kershaw EE, Hamm JK, Verhagen LA, et al. (2006) Adipose triglyceride
lipase: function, regulation by insulin, and comparison with adiponutrin.
Diabetes 55: 148-157.
- Camargo A, Meneses ME, Pérez-Martínez P, et al. (2014) Dietary fat
modifies lipid metabolism in the adipose tissue of metabolic syndrome
patients. Genes Nutr 9: 409.
- Fielding B (2011) Tracing the fate of dietary fatty acids: metabolic
studies of postprandial lipaemia in human subjects. Proc Nutr Soc 70:
342-350.
- van Hees AM, Jocken JW, Essers Y, et al. (2012) Adipose triglyceride
lipase and hormone-sensitive lipase protein expression in subcutaneous
adipose tissue is decreased after an isoenergetic low-fat high-complex
carbohydrate diet in the metabolic syndrome. Metabolism 61: 1404-1412.
- Jocken JW, Langin D, Smit E, et al. (2007) Adipose triglyceride
lipase and hormone-sensitive lipase protein expression is decreased in the
obese insulin-resistant state. J Clin Endocrinol Metab 92: 2292-2299.
- Verhoef SP, Camps SG, Bouwman FG, et al. (2013) Physiological
response of adipocytes to weight loss and maintenance. PLoS One 8: e58011.
- Demir B, Ucak H, Cicek D, et al. (2014) Changes in serum desnutrin
levels in patients with acne vulgaris. Eur J Dermatol.
- Yang L, Chen SJ, Yuan GY, et al. (2014) Association of serum adipose
triglyceride lipase levels with obesity and diabetes. Genet Mol Res 13:
6746-6751.
- Schon MP, Boehncke WHO (2005) Psoriasis. N Engl J Med 352:
1899-1912.
- Langin D, Arner P (2006) Importance of TNF alpha and neutral lipases
in human adipose tissue lipolysis. Trends Endocrinol Metab 17: 314-320.
-
 Table 1
Table 1 -
Table 2

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- International Journal of Anaesthesia and Research (ISSN:2641-399X)
- International Journal of Clinical Case Studies and Reports (ISSN:2641-5771)
- Journal of Immunology Research and Therapy (ISSN:2472-727X)
- Journal of Renal Transplantation Science (ISSN:2640-0847)
- Stem Cell Research and Therapeutics (ISSN:2474-4646)
- Ophthalmology Clinics and Research (ISSN:2638-115X)
- International Journal of Surgery and Invasive Procedures (ISSN:2640-0820)


