729
Views & Citations10
Likes & Shares
Hypertension continues to pose public health challenge in Nigeria, the
most populous Black Country. The interplay of obesity, overweight and hyperlipidemia
contribute to development of hypertension and other NCDs. This review includes
studies published between 2010 and 2018. Google Scholar and PubMed were the
search engines. Six studies were reviewed and each study comes from one of the
geopolitical zones of Nigeria. Overweight, obesity and dyslipidemia were common
among the Nigerian hypertensive patients. The relationship of overweight and
obesity to hypertension was confirmed. The relationship between dyslipidemia
and hypertension is uncertain in some parts of Nigeria. Overweight, obesity and
dyslipidemia are predictors of hypertension among the hypertensive outpatients
in Nigeria.
Keywords: Overweight, Obesity,
Hyperlipidemia, Hypertension
INTRODUCTION
Hypertension continues to pose public health challenge
in African countries where it is more prevalent than other continents in the
World. It accounts for 20.8 million cases in Nigeria, the most populous black
country among people aged 20 years and above in 2010 [1]. The interplay of
obesity, overweight and hyperlipidemia with their contribution to hypertension
and many other non-communicable diseases has been confirmed [2].
Hypertension is now on the increase in Nigeria where
adoption of western lifestyles and the stress of urbanization both of which are
expected to increase the morbidity associated with unhealthy lifestyles are
progressing [9]. According to some researchers, hypertension and dyslipidemia
account for more than 80% of deaths and disability in low- and middle-income
countries. The relationship between obesity and high blood pressure through the
anthropometric indexes in both clinical and population studies have been
confirmed among the Nigerian
Framingham and other epidemiological surveys as well
as experimental studies have shown that serum lipid abnormalities are not only
associated with hypertension, it significantly increases the risk for
cardiovascular disease and its complications. Fasae et al. [12] and
Tekes-Manova et al. [13] reported that dyslipidemia is the second most
prevalent cardiovascular risk factor. However, in order to address the menace
of obesity and dyslipidemia which are the risk factors of hypertension in a
country by appropriate policy studies from different regions of the country
need to be examined. This review examines the extent that obesity and
dyslipidemia influence on the prevalence of hypertension in Nigeria.
METHODS
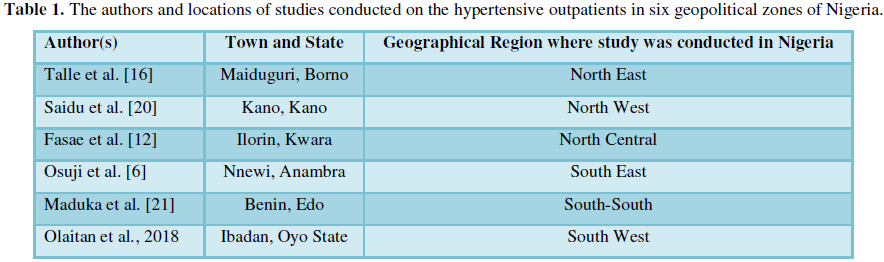
This review includes studies published between 2010 and April 23, 2018. The search terms used are nutritional status and lipid profile of hypertensive adults in Nigeria. Having the search to start from 2010 is to give allowance to cover all the studies done in the six regions of Nigeria. Six studies were reviewed and each study comes from each geopolitical zone of Nigeria (Table 1). In order to eliminate difficulty in analysis, only surveys which used BMI to measure the nutritional status and which conducted the lipid profile of the hypertensive adults were selected. Though there were studies which measured the waist circumference and waist-hip ratio but BMI is used as a reference for this review. Obesity is defined as a body mass index (BMI) equal or greater than 30 kg/m2 and overweight as BMI of 25 kg/m2 and more but less than 30 kg/m2 [14]. Serum lipid abnormalities were defined as elevated serum TC=5.2 mmol/l (=200 mg/dl); elevated serum LDL-c=3.37 mmol/l (130 mg/dl); elevated serum TG=1.7 mmol/l (=150 mg/dl); and low serum HDL-c<0.9 mmol/l (35 mg/dl) for males and <1.0 mmol/l (39 mg/dl) for females [10] Hypertension is defined by systolic blood pressure ≥ 140 mm Hg and diastolic blood pressure ≥ 90 mm Hg according to the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) classification [15].
Criteria for the inclusion of articles are as
follows:
1. The study should only involve hypertensive adults in Nigeria.
2. It should cut across at all the six geographical zones in
Nigeria.
3. The location of the study in Nigeria was stated.
4. BMI was used to determine overweight and obesity
5. Stratification of overweight and obesity was clearly spelt out.
6. The survey should involve both males and females.
7. The study should involve hypertensive adults whose lipid
profiles were assessed.
In instances where more than one survey was obtained
from a city or state, only the most recent study was included in the present
research.
RESULTS
The search on the nutritional status and lipid profile of the hypertensive adults in Nigeria was conducted on 20 abstracts but only six abstracts met the inclusion criteria and full survey were obtained from the internet with the use of Google Scholar and PubMed as search engines. The mean BMI of the hypertensive patients attending the tertiary health centres in Nigeria ranges from 26.55 ± 4.17 kg/m2 in Kano to 32.00 ± 8.20 kg/m2 in Benin (Table 2).
The mean SBP of the hypertensive patients ranges
from 143.32 ± 14.97 mm Hg in Kano to 163.3 ± 18.9 mm Hg in Nnewi. The mean DBP
of the hypertensive patients ranges from 86.76 ± 9.24 mm Hg in Kano to 106 ±
16.4 mm Hg in Ilorin. The mean elevated Total Cholesterol ranges from 4.64 ±
1.02 mmol/L in Maiduguri to 4.89 ± 0.93 mmol/L in Ibadan. The mean elevated
Triglyceride ranges from 0.96 ± 0.46 mmol/L in Benin to 2.93 ± 1.69 mmol/L in
Ibadan. The mean elevated Low density lipoprotein ranges 3.00 ± 0.82 mmol/L in
Nnewi to 3.1 ± 1.1 mmol/L in Kwara. The mean low High density lipoprotein
ranges 1.06 ± 0.29 mmol/L in Maiduguri to 1.36 ± 1.26 mmol/L in Kano (Table
3).
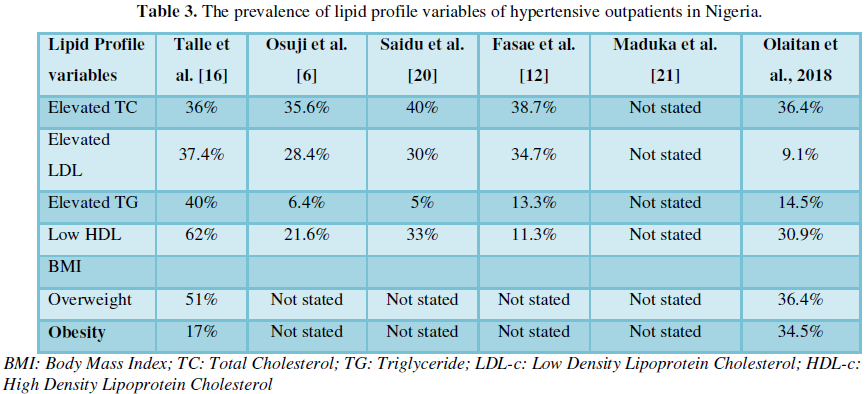
On the association of lipid profile and hypertension, all hypertensive outpatients in the reviewed studies demonstrated elevated mean serum total cholesterol except the patients in Benin. Positive correlation was observed between raised blood pressure and elevated serum total cholesterol and lower high density lipoprotein in the cross sectional study conducted among hypertensive outpatients in Ibadan. Significant higher LDL-C was observed only among hypertensive patients in Ilorin, Nnewi, Kano and Benin. Elevated serum TG was found to be significantly higher among the hypertensive patients in Nnewi, Kano and Benin. Lower serum HDL-C was found to be prevalent among the hypertensive patients in Ibadan, Kano, Maiduguri and Kano. Only and Osuji et al. [6] and Talle et al. [16] reported a positive correlation between BMI and all lipid profile variables except HDL-C. Certain researchers found no correlation between BMI and any of the lipid profile variables. But, other studies did not observe the association between BMI and lipid profile variables.
Discussion
This review studied the nutritional status (based on
Body Mass Index) and lipid profile of hypertensive patients attending the
tertiary hospitals in Nigeria. Previous systematic review conducted by
Chukwuonye et al. [17] reported the prevalence of overweight and obesity among
Nigerian adults to be 20.3%-35.1% for overweight and 8.1%-22.2% for obesity.
This review found prevalence of overweight among the hypertensive patients to
be within 36.4%-51% and obesity to range from 17.0%-34.5%. It was observed that
mean BMI among hypertensive outpatients in Nigeria ranges from 26.55 ± 4.17
kg/m2 to 32.00 ± 8.20 kg/m2. This confirms the reports of previous studies that
many of the hypertensive patients attending Nigeria tertiary hospitals are
still overweight and obese [10,18,19]. Prevalence of overweight and obesity
among the hypertensive patients in Nigeria reveals that majority of them are
suffering from diabetes and other metabolic disorders.
Positive correlation between hypertension and BMI
was observed in the studies conducted by Osuji et al. [6] and Saidu et al. [20]
in Nnewi and Kano. Maduka et al. [21] reported high prevalence of obesity among
hypertensive patients in Maiduguri, whereas, others reported high prevalence of
overweight among the hypertensive patients in Ibadan. In contrast, no
correlation was found between hypertension and BMI among hypertensive patients
in Benin and Ilorin [12,21] This review shows that relationship of hypertension
with overweight and obesity is uncertain in South-south and North Central of
Nigeria. Although, Idemudia [22] had earlier reported significant high BMI
among the hypertensive patients compared to normotensive individuals. Study
conducted by Gudlavalleti et al. [23] across different ethnic groups in Nigeria
also affirmed that hypertension increased with BMI but BMI is independently
associated with hypertension at p<0.001 and south-south had significant
higher odds ratio of hypertension than other geopolitical zones in
Nigeria.
Previous systematic review conducted revealed that
the prevalence of hypertension among adults in Nigeria ranges from 43.6% to
50.8%. This study found uncontrolled systolic blood pressure to range from
Grade 1 hypertension (143.32 ± 14.97 mm Hg) to Grade 2 systolic hypertension
(163.3 ± 18.9 mm Hg) and diastolic blood pressure ranges from high normal
(86.76 ± 9.24 mm Hg) to Grade 3 diastolic blood pressure (106 ± 16.4 mm Hg)
according to the classification of European Society of Hypertension and the
European Society of Cardiology (ESH/ESC). Although, the mean systolic BP among
the Nigerian hypertensive patients is lower than those in India, the mean
diastolic BP of Nigerian hypertensive patients is higher than theirs [24].
Having hypertensive patients with significant high
lipid profile in the reviewed studies confirms the result of previous studies
conducted both in Nigeria and abroad which reported close association between
raised blood pressure and dyslipidemia [25-27] show that Total cholesterol and
the mean of serum LDL level were significantly higher in the hypertensive
patients in Iran. Pyadala et al. [28] also reported a significantly higher TC,
TG, LDL and very LDL in hypertensive subjects that visited teaching hospital in
Sanga Reddy, India. However, hypertensive patients who have hyperlipidemia are
at risk of developing diabetes and kidney disease [2]
LIMITATIONS OF THE STUDY
This review has limitations in some areas. Many of
the studies reviewed used small sample size. Not all the studies measure the
association between BMI and lipid profile, BMI and hypertension and lipid and
hypertension. Many of the studies did not measure dietary intake and lifestyles
which could be the risk factors of dyslipidemia, overweight, obesity and
hypertension. These limitations could affect the generalizability of this
review to the condition of hypertensive outpatients in Nigeria.
CONCLUSION
It becomes evident that hypertensive outpatients in
Nigeria still demonstrate hypertension up to the isolated systolic
hypertension. Overweight, obesity and dyslipidemia are the predictors of the
high blood pressure in Nigeria. The association between hypertension and
dyslipidemia is uncertain in some parts of Nigeria. Many of the hypertensive
outpatients in Nigeria are suffering from other metabolic disorders along with
hypertension which could be diabetes, renal diseases or both. The patients
shows the tendency of suffering from cardiovascular diseases such as
atherosclerosis, heart diseases and stroke later in future if appropriate
measure is not put in place.
RECOMMENDATION
The physicians are
encouraged to assess the obesity and dyslipidemia among their hypertensive
patients, monitor the patients to weight loss and direct them to registered
dietitians for dietary regime to monitor their dietary intake which could
predispose them to hyperlipidemia. Government at all levels is encouraged to
provide financial support in the diagnostic procedures of hypertension which
could be costly for some hypertensive patients to do on their own.
1. Adeloye
D, Basquill C, Adewale A, Thompson YJ, et al. (2014) An estimate of the
prevalence of hypertension in Nigeria. J Hypertens 33: 230-242.
2. Behradmanesh
S, Nasri P (2012) Serum cholesterol and LDL-C in association with level of
diastolic blood pressure in type 2 diabetic patients. J Renal Inj Prev 1:
23-26.
3. Abubakar
A, Mabruok MAM, Gerie AB, Dikko AU, Aliyu S, et al. (2009) Relation of body
mass index with lipid profile and blood pressure in healthy female of lower
socioeconomic group, in Kaduna Northern Nigeria. Asian J Med Sci 1: 94-96.
4. Yasein
N, Ahmad M, Matrook F, Nasir L, Froelicher ES (2010) Metabolic syndrome in patients
with hypertension attending a family practice clinic in Jordan. East Mediterr
Health J 16: 37580.
5. The
European Food Information Council (2006) Obesity and overweight. Available
from: http://www.eufic.org/article/en/expid/basics-obesityoverweight/
6. Osuji
CU, Omejua EG, Onwubuya EI, Ahaneku GI (2012) Serum lipid profile of newly
diagnosed hypertensive patients in Nnewi, South-East Nigeria. Int J Hypertens
12: 1-7.
7. Ferrara
LA, Guida L, Iannuzzi R, Celentano A, Lionello F (2002) Serum cholesterol
affects blood pressure regulation. J Hum Hypertens 16: 337-343.
8. Aboyans
V, Lacroix P, Criqui MH (2007) Large and small vessels atherosclerosis:
Similarities and differences. Prog Cardiovasc Dis 50: 112-125.
9. FMOH
(2009) Ministerial Press briefing. Available at: http//www.fmoh.org.ng
10. Adedoyin
RA, Mbada CE, Bisiriyu LA, Adebayo RA, Balogun MO, et al. (2008) Relationship
of anthropometric indicators with blood pressure levels and the risk of
hypertension in Nigerian adults. Int J Gen Med 2008: 133-140.
11. Iloh
GUP, Amadi AN, Nwankwo BO, Ugwu VC (2011) Obesity in adult Nigerians: A study
of its pattern and common primary co-morbidities in a rural Mission General
Hospital in Imo state, south-eastern Nigeria. Nig J Clin Pract 14: 212-218.
12. Fasae
AJ, Busari OA, Opadijo OG, Omotoso AB (2015) Hyperuricaemia and its relations
with serum lipid abnormalities in untreated, newly diagnosed adult Nigerian
hypertensive patients. Br J Med Med Res 7: 779-788
13. Tekes-Manova
D, Israeli E, Shochat T, Swartzon M, Gordon S, et al. (2006) The prevalence of
reversible cardiovascular risk factors in Israelis aged 25-55 years. IMAJ 8:
527-531.
14. World
Health Organization (1995) Technical Report Series. Geneva, Switzerland: World
Health Organization.
15. Mancia
G, Fagard R, Narkiewicz K, Redón J, Zanchetti A (2013) ESH/ESC Guidelines for the management of arterial hypertension:
The Task Force for the management of arterial hypertension of the European
Society of Hypertension (ESH) and of the European Society of Cardiology (ESC).
J Hypertens 31: 1281-1357.
16. Talle
MA, Enyikwola O, Delaiye AA, Yusuph H, Baba MM, et al. (2010). Disorders of
lipids among newly diagnosed hypertensive patients in Maiduguri, northeastern
Nigeria. Borno Med J 1: 10-14.
17. Chukwuonye
II, Chuku A, Collins J, Arinze KO, Imoh ME, et al. (2013) Prevalence of overweight
and obesity in adult Nigerians – A systematic review. Diabetes Metab Syndr Obes
6: 43-47.
18. Akuyam
SA, Aghogho UB, Aliyu IS, Bakari AG (2009) Serum total cholesterol in
hypertensive northern Nigerians. Int J Med Med Sci 1: 73-78.
19. Aliyu
SU, Oyeyemi AY, Udoh DG, Oyeyemi AL (2014) Prevalence of overweight/obesity and
undiagnosed hypertension among military personnel in Maiduguri, Nigeria. J Nov
Physiother 5: 237.
20. Saidu
H, Karaye KM, Okeahialam BN (2014) Plasma lipid profile in Nigerians with
high-normal blood pressure. BioMed Central Res Notes 7: 930.
21. Maduka
IC, Osunbor JO, Osunbor AO, Egwu MC (2018) Evaluation of thyroid function and
lipid profile of hypertensive subjects. J Med Med Sci 6: 160-164.
22. Idemudia
JO (2014). Dyslipidaemia in hypertensive in south-south Nigeria. Br J Med Med
Res 4: 4742-4750.
23. Gudlavalleti
VSM, Samantha F, Selvaraj S, Clare EG, Abdull MM, et al. (2013). Prevalence and
risk factors for hypertension and association with ethnicity in Nigeria:
Results from A National Survey. Cardiovasc J Afr 24: 344-350.
24. Pooja,
Mittal Y, Mathur A (2013) Evaluation of lipid profile of north indian
hypertensive subjects. Asian J Biomed Pharm Sci 3: 38-41.
25. Nwosu
ZC, Edeogu OC (2011) Increased lipid profile in hypertensive Nigerian males: A
possible risk for atherosclerosis. Pak J Med Sci 27: 269-272.
26. Choudhury
KN, Mainuddin AKM, Wahiduzzaman, Shariful SM (2014) Serum lipid profile and its
association with hypertension in Bangladesh. Vasc Health Risk Manag 10:
327-332.
27. Ghooshchi
G, Masoomian M, Sarafraz Yazdi M, Pour Ramezan M (2014) Evaluation of the lipid
profile of hypertensive patients compared to non-hypertensive individuals.
Patient Saf Qual Improv 2: 120-122.
28.
Pyadala N, Bobbiti RR, Borugadda R,
Bitinti S, Maity SN, et al. (2017) Assessment of lipid profile among
hypertensive patients attending to a rural teaching hospital, Sangareddy. Int J
Med Sci Public Health 6: 71-74.
29. Olaitan OO, Fadupin GT, Adebiyi AA (2018) Dietarypattern, lifestyle and nutritional status of hypertensiveoutpatients attending University College Hospital,Ibadan, Nigeria. Afr J Biomed Res 21: 29-36.
-
 Table 1
Table 1 -
Table 2
-
Table 3